

mRNA Shots are Being Used in Pork. Soon, Cattle may Get mRNA Shots as well, which could Affect Beef and Dairy Products: Beef Producers Panic Over mRNA Vaccine News
/
STORY AT-A-GLANCE
Pork producers have been using customizable mRNA-based “vaccines” on their herds since 2018, without telling the public
All customized mRNA “vaccines” are untested. Only the mRNA platform itself has been approved
According to the National Cattlemen’s Beef Association, “there are no current mRNA vaccines licensed for use in beef cattle in the United States.” However, a lobbyist for the association claims to have “double-vaccinated” his own herd with an mRNA “vaccine” against bovine respiratory disease
Iowa State University began trialing an mRNA “vaccine” against bovine respiratory syncytial virus October 1, 2021
Missouri House Bill 1169 would require labeling of products that can alter your genes. Big Ag lobbyists strongly oppose it
From [MERCOLA] Last week, I reported that pork producers have been using customizable mRNA-based "vaccines" on their herds since 20181 — without telling the public. This issue really only rose to the surface after attorney Tom Renz started promoting new legislation in Missouri (House Bill 1169, 2 which he helped write) that would require labeling of mRNA products. 3 In an April 1, 2023, tweet (and no, this was not an April Fool's joke), Renz stated:4
"BREAKING NEWS: the lobbyists for the cattleman and pork associations in several states have CONFIRMED they WILL be using mRNA vaccines in pigs and cows THIS MONTH. WE MUST SUPPORT MISSOURI HB1169. It is LITERALLY the ONLY chance we have to prevent this … NO ONE knows the impacts of doing this but we are all potentially facing the risk of being a #DiedSuddenly if we don't stop this."
The Transhumanist Agenda and Its Focus on Food
Within days, alternative media was abuzz with this story and Renz started making the rounds sharing evidence that shows the U.S. government has been working on the integration of vaccines into foods for at least two decades. In an April 2, 2023, interview with Naomi Wolf, Ph.D., Renz said: 5
"[Bill] Gates, the WHO [World Health Organization], a ton of these universities: they're all talking about including mRNA vaccinations as part of the food. They're going to modify the genes of these foods to make them mRNA vaccines."
Industry Doesn't Want You to Know What They're Doing
The pushback by Big Ag lobbyists against this bill to require industry transparency on this important issue has been enormous, and one potential reason for that is because they'd have to admit that all sorts of foods may have been vaccinated with mRNA vaccines, have genetic modifications, or be modified to serve as vaccinations for humans.
Not only might this destroy Big Ag, but it would also seriously impact any surreptitious attempts by Big Pharma to use the food supply as a tool to distribute vaccines unbeknownst to consumers. 6
In short, Renz suspects the globalists' transhumanist agenda is being secretly pushed forward using gene therapy in food production.
I can't help but wonder whether the industry simply doesn't understand how mRNA gene therapy in livestock might affect consumers, or whether they want to conceal the fact that they're using gene therapy because they DO know it can also affect humans.
Globalists like World Economic Forum founder Klaus Schwab have openly admitted that they intend to alter humanity — both on the genetic level and through the incorporation of artificial intelligence and nanotechnology into the human body.
And, using COVID-19 as the cover, they managed to turn the entire world population into test subjects for this dangerous experimentation. As noted by Renz in the Real America's Voice interview above, we know for a fact that the mRNA COVID shots have no beneficial impact in terms of preventing COVID infection.
mRNA 'Vaccines' in Livestock Are Untested
If the mRNA COVID shots don't prevent infection, why would we assume mRNA shots for viral and bacterial infections in swine work any better?
One of the most disturbing aspects of using mRNA "vaccines" in swine is the fact that all of them are by definition untested. As explained by Merck on its website, its "custom swine vaccine," Sequivity, is not a vaccine but, rather, a platform that allows for the endless customization of "mRNA vaccines."
The customized mRNA shots that are created using it are completely untested. Here's how it works: 7
A pathogen is collected and sent to a diagnostic lab.
The gene of interest is sequenced and sent electronically to Sequivity analysts.
A synthetic version of the gene of interest is synthesized and inserted into the RNA production platform.
The RNA particles released from incubated production cells are harvested and formulated into a customized "vaccine."
As noted by Zoetis, the largest producer of veterinary drugs and vaccines: 8
"Sequivity has safety and efficacy studies based on the platform with a historical initial isolate, not likely the isolate that customers would be requesting in their product."
What was that initial isolate? Will mRNA against a bacterial disease affect the animals in the same way that mRNA against a viral infection does? What "genes of interest" are being chosen? If spike proteins are selected, might they be as pathogenic as the SARS-CoV-2 spike protein?
In CAFO environments with high populations of animals, won't mutations become rampant as the bacteria and viruses are subjected to constant "customized" vaccination pressure to adapt and become more dangerous? These are just some of the questions that need answers.
At the end of the day, the fact that mRNA shots can be endlessly customized without safety testing shows just how broken the U.S. Department of Agriculture and the Food and Drug Administration are.
There's simply no way they can guarantee that customized mRNA shots are safe. The fact that the platform itself works and allows for this customization does NOT prove the safety and effectiveness of the shots being cooked up. Approval of the platform also does not prove the food is safe for consumption after it's been treated with mRNA.
Cows Milk Used to Immunize Mice
As reported by Dr. Peter McCullough, 9 Chinese researchers have demonstrated that food can indeed be turned into a vaccine. 10
"The nation's food supply can be manipulated by public health agencies to influence population outcomes … Now an oral route of administration is being considered specifically for COVID-19 vaccination using mRNA in cow's milk.
Zhang and colleagues have demonstrated that a shortened mRNA code of 675 base pairs could be loaded into phospholipid packets called exosomes derived from milk and then using that same milk, be fed to mice.
The mice gastrointestinal tract absorbed the exosomes and the mRNA must have made it into the blood stream and lymphatic tissue because antibodies were produced in fed mice against SARS-CoV-2 Spike protein (receptor binding domain) …
[G]iven the damage mRNA vaccines have generated in terms of injuries, disabilities, and deaths, these data raise considerable ethical issues. The COVID States project has shown that 25% of Americans were successful in remaining unvaccinated.
This group would have strong objections to mRNA in the food supply, particularly if it was done surreptitiously or with minimal labelling/warnings …
For those who have taken one of the COVID-19 vaccines, having milk vaccines as an EUA offering would allow even more loading of the body with synthetic mRNA which has been proven resistant to ribonucleases and may reside permanently in the human body.
These observations lead me to conclude that mRNA technology has just entered a whole new, much darker phase of development. Expect more research on and resistance to mRNA in our food supply. The Chinese have just taken the first of what will probably be many more dangerous steps for the world."
Will Beef Be Treated With mRNA Too?
At present, there's no evidence to suggest beef cattle are being treated with customizable mRNA "vaccines," either in Europe 11 or the U.S. The National Cattlemen's Beef Association has also denied it, saying "there are no current mRNA vaccines licensed for use in beef cattle in the United States." 12 13
That said, the Cattlemen's Association previously confirmed they do, eventually, intend to use mRNA shots in cattle, 14 15 which might affect both dairy and beef. Time will tell whether public outrage will halt such plans. Clearly, the Cattlemen's Association is concerned about internet rumors that it's already in use.
April 3, 2023, Texas Department of Agriculture commissioner Sid Miller issued a statement promising to conduct a risk assessment of the technology before its adoption: 16
"Since news of the development of mRNA vaccines and mRNA-related treatments for livestock came to the attention of the Texas Department of Agriculture, we have been working towards developing a fact and science-based assessment of the risks associated with this technology.
Our analysis will include the clinical research, the structure of existing Texas law, and the public policy, economic, and production impact of the different policy prescriptions we may adopt. I aim to ensure that Texas agriculture remains safe, trusted, healthy, and wholly uninfected by dangerous or unproven technology.
I personally take this issue very seriously. No political hot takes. Just a well-reasoned and well-researched proposal based on a wide range of input from stakeholders, scientists, agriculturalists, and other experts. We are looking at this issue at TDA and will share your concerns. Please stay tuned …"
Confusion Caused by Cattlemen's Association Lobbyist
What's causing significant confusion on this issue is a statement made by National Cattlemen's Beef Association lobbyist Shannon Cooper 17 before the Missouri House. 18
Cooper told the House members he had recently "double-vaccinated" his herd with "vaccinations that have this mRNA." According to Cooper, the mRNA "vaccine" given was for bovine respiratory disease.
Is he confused? Did he mistakenly believe the vaccine he gave had mRNA in it? Or is the National Cattlemen's Beef Association incorrect in stating there are no approved mRNA vaccines for cattle in the U.S.? Or, are experimental mRNA shots being used without approval? Who knows at this point?
What we do know is that mRNA "vaccines" against bovine respiratory disease are being developed. Iowa State University began trialing an mRNA "vaccine" against bovine respiratory syncytial virus October 1, 2021.19
The project end date is listed as September 30, 2026.
According to the trial submission, mice would be used to establish proof of concept. Cows would be used in year two of the trial. Assuming they're on schedule, that means cows will be experimented on somewhere in late 2023 and/or 2024.
Is mRNA Jabbed Livestock Safe to Eat?
Considering health authorities insist the COVID shots are safe, it's no wonder they also insist there are no problems associated with eating mRNA-treated meat. But can we trust them? What about the cells now highjacked by the foreign mRNA instruction to create novel proteins? Are these proteins safe to consume? How long are the nano-lipid particles preserved in the tissue?
Livestock such as swine are routinely vaccinated against several diseases, 20 and many of these vaccines must be administered at specific times to ensure there's no residue left in the meat. So, just when are swine receiving these customized mRNA shots? And could there be mRNA vaccine remnants in the pork you buy?
Vaccines are nearly always given in the hindquarter of the animal, and according to mRNA jab developers, the mRNA remains at the injection site. This theory has long since been proven false, as the mRNA in the COVID jab gets has been shown to be distributed throughout the human body.
But it makes sense that the mRNA might be more concentrated at the injection site. In livestock, this could be bad news, seeing how the hindquarters are usually where the prime cuts of meat come from.
So, knowing whether there's any mRNA left in the animal at the time of slaughter is important. At present, we have no way of knowing this. We don't even know exactly how long the synthetic lipid-enveloped mRNA stays in the body.
We also don't know how long the antigen produced by the animal's cells in response to a customized mRNA shot sticks around, and whether ingesting that antigen might have repercussions for human health.
Stanford researchers found the spike protein produced in response to the COVID shot remains in the human body for at least 60 days, 21 22 and the spike protein is what's causing most of the health problems associated with the jab. Could the same be true for mRNA jabs used in animals? Hogs can be killed anywhere from the age of 6 weeks to 10 months, which doesn't allow a whole lot of time for the mRNA and/or antigen to get flushed out. 23
Notorious Industry Mouthpiece Defends Livestock mRNA Jabs
Aside from the many open questions, the fact that notorious Big Pharma mouthpieces are the ones cited by media, ensuring us that mRNA jabbed animals are safe to eat is yet another red flag. In this case, we have Dr. Kevin Folta insisting the mRNA is harmless.
Folta, a University of Florida horticulture professor, is a longtime advocate for genetically modified organisms (GMOs). He has also advocated for the safety of glyphosate, and in 2015, he was caught lying about his financial ties to Monsanto. Now, he's taken up the advocacy for mRNA shots in livestock. As reported by Cowboy State Daily: 24
"Lawmakers in Arizona, Idaho, and Missouri have introduced legislation related to the use of mRNA vaccines in food. The Arizona bill only restricts labeling such food as organic. The Idaho bill amends state law to prohibit the sale of such foods unless conspicuously labeled that the presence of the vaccine is in the food.
The Missouri bill requires a conspicuous 'Gene Therapy Product' label. Dr. Kevin Folta told Cowboy State Daily the proposed 'gene therapy' label is inaccurate.
It 'means they have no idea what they are trying to regulate,' Folta said, because 'there is no integration into the DNA. It's a transient set of instructions, like a USB drive. Not a hard drive' … Messenger RNA occurs naturally as part of the function of cells in the body. 'mRNA is everywhere, and you cant live without mRNA,' Folta said …
Folta said that the vaccines can't get into the food people eat. 'mRNA is an extremely unstable molecule. That's why it works. It's very temporary. So when an animal is slaughtered or when a plant dies, mRNA is the first thing to go,' Folta said."
Many of you will know exactly what's wrong with Folta's arguments that mRNA is "everywhere" and therefore harmless, and that its activity is temporary because it's so unstable. The mRNA in the shots is synthetic and does NOT break down the way normal mRNA does.
He is clearly misleading people, and it's hard to believe it's not intentional, considering the fact that everyone who knows even the slightest bit about mRNA jab technology knows the synthetic mRNA has been designed to prevent rapid breakdown and is further stabilized by the nanolipid. So, Folta's arguments are null and void from the get-go.
Final Thoughts
Moving forward, it's going to be extremely important to stay on top of what's happening to our food supply. Many of us were surprised to realize mRNA shots have been used in swine for several years already. Soon, cattle may get these customizable mRNA shots as well, which could affect both beef and dairy products.
For now, I strongly recommend avoiding pork products. In addition to the uncertainty surrounding these untested mRNA "vaccines," pork is also very high in linoleic acid, a harmful omega-6 fat that drives chronic disease. Hopefully, cattle ranchers will realize the danger this mRNA platform poses to their bottom-line and reject it. If they don't finding beef and dairy that has not been "gene therapied" could become quite the challenge.
Will Harris, from White Oak Pasture in Bluffton Georgia, is a rancher who has already come out against mRNA "vaccines" in cattle. An April 10, 2023, White Oak Pastures tweet stated: 25
"There is talk about domesticated food animals soon being vaccinated with mRNA. We want our customers to know that we will not vaccinate our animals with mRNA vaccines. We believe there is a time and place for vaccinations, but they must be used sparingly.
If livestock are raised in an environment where they can express their natural instincts, they probably wont need many (if any) vaccines. We hope to one day move away from all vaccines on our farm — we are close, but not there yet.
Everyone should know that over 80% of the antibiotics produced today are consumed by domesticated food animals … It would only make sense that in order for vaccine companies to move from 'very profitable' to 'obscenely profitable' would be to capture the animal agriculture market.
I'm not sure that this would ever pass legislation, but law or not, Big Ag is highly influenced by Big Pharma. The multinational meat companies would certainly choose to mandate this if there was an opportunity for a shared profit.
In closing, please know: We don't believe in a blanket, one-size-fits-all approach to our health or our livestock. We will not add vaccinations for our livestock — we are moving in the other direction hoping to give fewer. (And, we already give very few).
If this is adopted and there is a 'panic' for food from livestock that hasn't had the MRNA vaccine, we will choose to honor the demand from our loyalty members and employees first. If you are not a part of that group, we cannot guarantee we will have any product for you.
We are certainly not trying to promote panic — but, we do intend to notify our customers of how we will operate in times of growing demand. We screwed up during the pandemic — we won't do that again."
Dr McCullough says Chinese Researchers have Demonstrated that Food can be Turned into a “Vaccine.” Authorities May Allow Big Agriculture to Put COVID mRNA “Vaccines” in the Food Supply
/From Peter A. McCullough, MD, MPH The nation’s food supply can be manipulated by public health agencies to influence population outcomes. A great is example is fortification of cereal grains with folic acid — the synthetic form of folate — which successfully reduced the incidence of neural tube defects (e.g. spina bifida). Now an oral route of administration is being considered specifically for COVID-19 vaccination using mRNA in cow’s milk.
Zhang and colleagues have demonstrated that a shortened mRNA code of 675 base pairs could be loaded into phospholipid packets called exosomes derived from milk and then using that same milk, be fed to mice. The mice gastrointestinal tract absorbed the exosomes and the mRNA must have made it into the blood stream and lymphatic tissue because antibodies were produced in fed mice against SARS-CoV-2 Spike protein (receptor binding domain).
An oral vaccine for SARS-CoV-2 RBD mRNA-bovine milk-derived exosomes induces a neutralizing antibody response in vivo. Quan Zhang, Miao Wang, Chunle Han, Zhijun Wen, Xiaozhu Meng, Dongli Qi, Na Wang, Huanqing Du, Jianhong Wang, Lu Lu, Xiaohu Ge bioRxiv 2022.12.19.517879; doi: https://doi.org/10.1101/2022.12.19.517879
From a scientific perspective, these experimental steps taken by the Chinese were a stunning success. However, given the damage mRNA vaccines have generated in terms of injuries, disabilities, and deaths, these data raise considerable ethical issues. The COVID States project has shown that 25% of Americans were successful in remaining unvaccinated. This group would have strong objections to mRNA in the food supply, particularly if it was done surreptitiously or with minimal labelling/warnings. Children could be targeted with easily administered oral vaccine dosing or potentially get mRNA through milk at school lunches and other unsupervised meals.
For those who have taken one of the COVID-19 vaccines, having milk vaccines as an EUA offering would allow even more loading of the body with synthetic mRNA which has been proven resistant to ribonucleases and may reside permanently in the human body.
These observations lead me to conclude that mRNA technology has just entered a whole new, much darker phase of development. Expect more research on and resistance to mRNA in our food supply. The Chinese have just taken the first of what will probably be many more dangerous steps for the world.
If you find “Courageous Discourse” enjoyable and useful to your endeavors, please subscribe as a paying or founder member to support our efforts in helping you engage in these discussions with family, friends, and your extended circles.
Former Director of National Intelligence Admits Fauci Lied about Gain of Function Research
/
From [HERE] While testifying before Congress this week, former Director of National Intelligence (DNI) John Ratcliffe told legislators that former head of the National Institute of Allergy and Infectious Diseases (NIAID) Tony Fauci lied under oath about the gain of function research that was taking place on the Wuhan coronavirus (Covid-19) prior to its release.
Appearing before the House Select Subcommittee on the Coronavirus Pandemic, Ratcliffe was questioned by Rep. Nicole Malliotakis (R-N.Y.) about Fauci’s infamous sworn testimony before the Senate back in November of 2021. Fauci told Sen. Rand Paul (R-Ky.) at the time that the NIH, which oversees the NIAID, did not fund any gain of function research.
(Related: Former National Institutes of Health [NIH] director Francis Collins also lied about gain of function research and other elements of the covid scamdemic.)
Rep. Malliotakis revealed that Fauci knew, as he was told in an email dated from January of 2021, that the NIH had, in fact, formed a monetary relationship with the Wuhan Institute of Virology through the EcoHealth Alliance, which was, in fact, conducting gain of function research in communist China using American taxpayer dollars.
“Some of Dr. Fauci’s testimony is inconsistent with some of the intelligence that we have that remains classified as well as inconsistent with some information that is publicly available,” Ratcliffe responded carefully to Rep. Malliotakis’ questioning – watch below:

Fauci lied; many people died
Gain of function research, just to get you back up to speed, involves modifying pathogens like coronaviruses with the intent of making them deadlier or more transmissible. The claim is that such research needs to be done in order to ascertain future pandemic threats, or so we are told.
In truth, it appears that a few mad scientist psychopaths embedded within the highest agencies of government commissioned such research overseas, since it is illegal stateside, for the purpose of creating a deadly bioweapon that they could then unleash upon the world.
Domestic funding for gain of function research dried up in 2014 when Barack Hussein Obama was president due to the risks involved. It was at that time that gain of function research appears to have been outsourced to overseas locations in order to sidestep that ban.
Around 2017, the NIH lifted Obama’s funding “pause” following the creation of a special oversight framework. American taxpayer dollars were then sent overseas for the purpose of manipulating bat coronaviruses in Wuhan, which is where the Wuhan coronavirus (Covid-19) is believed to have originated.
In his earlier defenses, Fauci tried to claim that the work being done at the Wuhan lab did not constitute gain of function research. This was denied by Dr. Richard Ebright, who clarified that the experiments taking place in Wuhan did, in fact, constitute gain of function research.
To this very day, the Biden regime still openly supports gain of function research, despite widespread concerns about the risks involved. Back in February, National Security Council communications coordinator John Kirby stated that Biden “believes that [the research is] important to help prevent future pandemics.”
Congress, meanwhile, continues to probe gain of function research to try to figure out whether or not the “lab leak” hypothesis is the most likely explanation for covid’s release.
COVID Injections and the Virus Itself Cause Neurological Disorders — But There’s a Difference, Study Says
/From [HERE] I stumbled upon this article in mainstream media, which linked to the Medpage Today review of an important study detailing functional neurologic disorders (FND) after COVID-19 infection or vaccination.
I don’t usually bother to re-publish items from Medpage Today because of their extreme bias against physicians and scientists who have spoken out about the pseudo-mRNA vaccine. I am making an exception because they actually published this review without bias.
I am posting sections of the article here for educational purposes only.
Please note the subtitle from Medpage article below, “Long COVID functional manifestations differ from post-vaccine effects.”
Within the body of the text, Medpage admits adverse events from the vaccine are more common than previously thought! Is this evidence that the tide of misinformation from medical journals geared toward physician education may be decreasing? One can only hope …
In my experience, post-vaccination twitching is almost as common as tinnitus (ringing in the ears). Based on this casual observation, I suspect that post-vaccination FND is quite common, which (if true) is likely to predict long-term neurologic consequences for a large fraction of the population.
According to “Functional Neurological Disorder Emerges After COVID Infection, Vaccines — Long COVID functional manifestations differ from post-vaccine effects,” Medpage Today, March 24, 2023:
“Patients with functional neurologic disorder (FND) after SARS-CoV-2 infection had different symptoms than people with FND after COVID vaccines, retrospective data showed.
“Patients with post-COVID FND tended to be older, had more insidious onset, and had higher disability, according to Araceli Alonso-Canovas, MD, PhD, of Hospital Universitario Ramón y Cajal in Madrid, and co-authors.
“Those with FND after COVID vaccination more closely resembled classic FND: they were younger, had an acute onset, and tremor was the most common phenotype, the researchers reported in Journal of Neurology, Neurosurgery & Psychiatry.
“‘We show for the first time evidence from a multicenter national study that FNDs after COVID-19 infections and vaccines are more common than previously reported and have distinct clinical profiles,’ Alonso-Canovas told MedPage Today.
“The findings point to a need to consider FND when diagnosing patients with post-COVID neurologic symptoms, she added.
“’Long COVID is an umbrella term and many different circumstances have to be considered,’ Alonso-Canovas said. ‘If there are neurological symptoms, a careful history and examination is mandatory to rule out FND, as it is a well-defined clinical condition that is potentially treatable.’
“FND refers to disorders caused by an abnormality in brain signaling with no significant structural brain damage. It occurs in an estimated four to 12 people per 100,000 per year and accounts for about 6% of outpatient neurology visits.
“Vaccinations can trigger FND, as can other stressors including infections. While experts maintain some people with FND might be long COVID patients, little research has been conducted to evaluate this.
“’If the neurological examination is not searching for these features, the diagnosis will be missed,’ Espay told MedPage Today. ‘Given the therapeutic implications, ascertaining the functional subtype of long COVID is imperative.’
“Phenotype was purely motor in 65% of FND patients and mixed sensorimotor in 32%. One patient had isolated sensory syndrome. Fatigue (72%), pain (57%), and cognitive difficulties (30%) were common.
“People in the post-COVID group were older (46 vs 35 years in the post-vaccine group) and had higher disability (76% vs 31%, respectively). The post-COVID group also trended toward having more men (24% vs 15%), more people with previous psychological difficulties (50% vs 23%), and less frequent abrupt FND onset (38% vs 62%).
“In the post-COVID group, 58% had previously received a long COVID diagnosis, and FND symptoms started within the convalescence period in 87% of patients. In the post-vaccine group, FND symptoms started within 1 week after vaccination in most cases.
“Overall, 22 FND patients (48%) required treatment with psychiatry or psychology specialists, 15 (33%) needed physical therapy, and one needed speech therapy. After a mean follow-up of 14 months from onset, 46% had improved, 39% remained stable, and 9% had worsened. Three patients were unavailable for follow-up after diagnosis.”
The actual scientific article may also interest readers, therefore highlights from that are posted below. Again, the main article is behind a paywall.
“Functional neurological disorders after COVID-19 and SARS-CoV-2 vaccines: a national multicentre observational study,” Journal of Neurology, Neurosurgery & Psychiatry, a BMJ Journal. [MORE]
Pfizer, CDC Withheld Evidence of Myocarditis After COVID Shots, New Documents Reveal. Dependent Media Conceals Story on Behalf of Their Masters
/
From [HERE] Pfizer and the Centers for Disease Control and Prevention (CDC) withheld evidence that COVID-19 vaccinations led to an increased risk of myocarditis, especially in young males, according to two sets of documents made public this week.
Confidential Pfizer documents leaked Thursday by Project Veritas show the company had “evidence that suggests patients who receive a COVID-19 vaccine are at an increased risk of myocarditis.”
And heavily redacted CDC documents obtained by Children’s Health Defense (CHD) via a Freedom of Information Act (FOIA) request indicate the agency provided an undercounted figure of post-COVID-19-vaccination myocarditis cases to Israel’s Ministry of Health in early 2021.
The latest revelations come as Germany, Japan and other governments are raising questions about the significant numbers of severe adverse events recorded in individuals following administration of the COVID-19 vaccines.
According to researchers at the National Organization for Rare Disorders, myocarditis can result from infections, or it may result directly from a toxic effect such as a toxin or a virus.
“More commonly the myocarditis is a result of the body’s immune reaction to the initial heart damage,” researchers said.
Severe myocarditis can permanently damage the heart muscle, possibly causing heart failure.
Internal documents contradict Pfizer claim of ‘low incidence of myocarditis’
An internal Pfizer document leaked to Project Veritas on Thursday, updated Feb. 11, 2022, and authored by eight scientists in Pfizer’s Drug Safety Research & Development division, indicates that the drugmaker was aware of a connection between mRNA COVID-19 vaccines and higher incidence rates of myocarditis within two weeks of vaccination — particularly following the second dose of the primary series.
“There is evidence that suggests patients who receive a COVID-19 vaccine are at an increased risk of myocarditis,” the document read.
“Onset was typically within several days after mRNA COVID-19 vaccination (from Pfizer or Moderna), and cases have occurred more often after the second dose than the first dose.”
Pfizer cited CDC data to make this determination:
“Since April 2021, increased cases of myocarditis and pericarditis have been reported in the United States after mRNA COVID-19 vaccination (Pfizer-BioNTech and Moderna), particularly in adolescents and young adults (CDC 2021).”
“The pattern of cases conform, as per the label, to a pattern of myocarditis cases occurring in majority of young males below 29 years of age within the first two weeks post-vaccination.”
“The reasons for male predominance in myocarditis and pericarditis incidence post COVID-19 vaccination remain unknown.”
Although Pfizer couldn’t identify a “clear mechanism” behind the increased risk in males, it did identify several possibilities.
These included direct cardiotoxicity, acute/active viral infection, genetic predisposition and pre-existing conditions, a prior history of myocarditis, immune-mediated mechanisms and vaccine-associated autoimmunity, molecular mimicry to the spike protein and sex-related effects.
These cases occurred, according to the document, despite a claimed low incidence of myocarditis during the clinical trials for the mRNA COVID-19 vaccines.
“Within the participants 16 years of age and older from the Pfizer clinical trial dataset, two cases of pericarditis were reported through the data cut-off date of 18 June 2021,” the document read. “These cases originated from the Phase 3 clinical study C4591001 and both were deemed not related to study treatment by the Investigator.”
“There were no cases of myocarditis reported as serious adverse events through the data cut-off date of 18 June 2021,” the document added.
Based on these incidences of myocarditis, the document states the product labels for the Pfizer COVID-19 vaccine were updated to state:
“Post marketing data demonstrate increased risks of myocarditis and pericarditis, particularly within 7 days following the second dose of the 2-dose primary series.
“The observed risk is higher among males under 40 years of age than among females and older males. The observed risk is highest in males 12 through 17 years of age.”
This change had already been made as of August 2021, according to a document released as part of the so-called “Pfizer documents” — documents pertaining to the U.S. Food and Drug Administration’s (FDA) issuance of Emergency Use Authorization (EUA) to the Pfizer-BioNTech COVID-19 vaccine.
The “Pfizer documents” were released last year by court order following a FOIA request filed by Public Health and Medical Professionals for Transparency.
Another internal Pfizer document from these same “Pfizer documents” states that on July 13, 2021, it was suggested that myocarditis and pericarditis be added “to the PVP” (pharmacovigilance plan).
This addition appears to have taken place.
The Pfizer pharmacovigilance plan of July 28, 2021 — also contained within the “Pfizer documents” release — lists myocarditis and pericarditis as “important identified risk[s]” identified in Pfizer’s safety database on June 18, 2021.
A pharmacovigilance plan “proposes activities to better characterize and assess the risks during the lifecycle of a medicine. (e.g., to investigate frequency, severity, seriousness and outcome of a risk under normal conditions of use, and/or which populations are particularly at risk).”
Pfizer’s July 28, 2021 pharmacovigilance plan stated that two serious adverse events of pericarditis were reported during the C4591001 clinical trial, although “both [were] deemed not related to study treatment by the Investigator.”
The document also refers to data from Pfizer’s safety database, stating that among people 16 and older, “490 cases reported events related to myocarditis and 371 cases reported events related to pericarditis (in 38 of these 823 cases, the subjects developed both myocarditis and pericarditis related events).”
Of these 490 cases, 26 were later definitively rejected as not being myocarditis, leaving 464 cases ranging from “definitive case” to “reported event.” From there, 459 were listed as “serious,” 337 required hospitalization, and 14 resulted in death.
Nearly 71% of these cases were recorded in males.
Of 371 reported pericarditis cases in individuals 16 and over, all but one was listed as “serious,” 206 required hospitalization, and 3 resulted in death.
Pfizer, in the same pharmacovigilance plan, claimed that no myocarditis or pericarditis cases were recorded in C4591001 trial participants ages 12 to 15.
However, its safety database recorded 11 possible cases of myocarditis — all but one among males, 10 of which were “serious” and nine of which required hospitalization.
Four cases of pericarditis among males between the ages of 12 and 15 also were recorded in the safety database, three of which were considered serious and one of which required hospitalization.
However, in the July 28, 2021 pharmacovigilance plan, Pfizer told the FDA:
“Considering the low rates of myocarditis and pericarditis reported following vaccination, balanced with the risk of death and illness (including myocarditis) caused by SARS-CoV-2, the public health impact of post-vaccination myocarditis and pericarditis is minimal.”
Nevertheless, in another leaked document publicized by Project Veritas, dated May 2022, further confirms Pfizer was aware of the increased incidence of myocarditis.
According to the leaked document:
“Adverse events (AEs) following COVID-19 vaccination are of high clinical importance: even adverse events with small incidence may be seen in appreciable numbers given the massive scope of the vaccination effort.
“There is evidence that suggests patients who received a COVID-19 vaccine are at an increased risk of myocarditis.”
CDC undercounted myocarditis cases in 2021
Documents provided by the CDC in response to an Oct. 12, 2022 FOIA request submitted by CHDreveal the agency provided an undercounted number of recorded myocarditis cases following COVID-19 vaccination to the Israeli Ministry of Health.
The FOIA request asked the CDC to “provide all emails sent by any of the relevant individuals or received by any of the relevant individuals (whether directly or via cc or bcc) containing the search word ‘myocarditis’” between Oct. 1, 2020 and April 30, 2021.
“There has been considerable public discussion of and controversy about how to weigh
the risk of myocarditis that is associated with COVID-19 vaccines,” the request stated. “The public has a significant interest in having a full understanding of how U.S. public health agencies have addressed this issue.”
Following a response by the CDC, CHD on Nov. 17, 2022, narrowed down its request to include only documentation containing the term “myocarditis” within 25 words of “(covid or report* or child* or adolescent* or young*or teen* or male or fatal* or death* or die* or serious or severe or hospital*).”
The heavily redacted 985-page tranche of documents provided to CHD included a Feb. 28, 2021 request, on page 692, from Israel’s Ministry of Health. The request, logged on that date by CDC’s internal task tracking system, stated:
“We are seeing a large number of myocarditis and pericarditis cases in young individuals soon after Pfizer COVID-19 vaccine. We would like to discuss the issue with a relevant expert at CDC.”
A CDC email, dated March 10, 2021, and found on pages 710-714 of the document, read:
“They are investigating a safety signal of myocarditis/myopericarditis in a younger population (16-30 years old) following administration of Pfizer-BioNTech COVID-19 vaccine.
“The Ministry of Health stated they received reports of around 40 cases of this adverse event.”
In the March 10, 2021 response, page 861, sent by the CDC to the Israeli Ministry of Health stated:
“A search of the U.S. Vaccine Adverse Event Reporting System (VAERS) conducted on February 23, 2021 revealed 27 cases (6 cases of myocarditis, 7 cases of myopericarditis, 14 cases pericarditis).
“Twelve cases occurred after dose 1, 7 cases after dose 2, and the dose was not reported for 8 cases. Four patients had comorbid conditions that could suggest alternate etiologies for the adverse event.
“During this analysis period the reporting rate of myopericarditis following administration of the mRNA COVID-19 vaccines was low and estimated to be 0.7 per million doses of vaccine administered.
“However, the limitations of passive surveillance such as under-reporting, lack of a control group, missing and incomplete data make it challenging to assess causation.
“Thus, FDA has not made a final determination regarding the causality between myopericarditis and the mRNA COVID-19 vaccines.”
However, up to Feb. 23, 2021, VAERS had actually received 36 reports of myocarditis — although at that time, the database was significantly backlogged.
It is unclear why data from a Feb. 23, 2021 search was provided by the CDC, when the request from Israel’s Ministry of Health was submitted on Feb. 28, 2021. There is no indication that there was contact from the Israeli health ministry with the CDC regarding this issue prior to Feb. 28, 2021.
While reports submitted to VAERS require further investigation before a causal relationship can be confirmed, the system has been shown to report only 1% of actual vaccine adverse events.
Studies have found further deficiencies in the VAERS system, including deleted or missing reports, the delayed entry of reports and the “recoding of Medical
Dictionary for Regulatory Activities (MedDRA) terms from severe to mild.”
Out of the deleted or missing reports, 13% pertained to deaths and 63% represented severe adverse events.
VAERS data is publicly accessible on the internet and presumably would already have been available to the Israeli Health Ministry as a result, therefore it is unclear why the CDC appears to have relied on this data in its response to Israel.
Moreover, by March 10, 2021, the presumed date of the CDC response to the Israeli Health Ministry, 14 more cases of myocarditis were reported to VAERS, for a total of 49 such cases identified in the database.
Of the 36 myocarditis cases reported to VAERS by Feb. 23, 2021, 25 were in males, 21 involved the Moderna vaccine (15 males), and 15 involved the Pfizer-BioNTech vaccine (10 males).
And of the 49 cases recorded by March 10, 2021, 35 were in males, 26 involved the Moderna vaccine (20 males) and 23 involved the Pfizer-BioNTech vaccine (15 males).
The average age of the patients was 33.6 and median age was 31.5 — with the average age of male cases being 31.1 (median 28) and the average age of females 40.8 (median 36.5), indicating a higher incidence in younger males.
The average number of days before onset and diagnosis following vaccination was 5.4, with a median of 3 days.
With hundreds of pages’ worth of redactions, it is unclear if there are more documents or data that would provide further insights into the response provided by the agency to Israel’s Ministry of Health.
In its Feb. 24 response, the CDC claims the redacted documents are protected by statute, confidentiality laws or privacy laws.
Notably, on the same day as the Israel Ministry of Health’s request to the CDC, Pfizer published a document — released as part of last year’s “Pfizer Documents” release from the FDA — titled “Cumulative Analysis of Post-Authorization Adverse Event Reports of PF-07302048 (BNT162B2) received through 28-Feb-2021.”
BNT162B2 refers to the Pfizer-BioNTech COVID-19 vaccine that received Emergency Use Authorization from the FDA.
This document indicated that 25 cases of myocarditis were reported by Feb. 28, 2021 as part of a list of “adverse events of special interest” (AESI).
This figure drew from several databases, including the Brighton Collaboration (SPEAC), the EU’s ACCESS protocol, U.S. CDC (preliminary list of AESI for VAERS surveillance) and the UK’s Medicines and Healthcare Products Regulatory Agency.
Studies show COVID shots lead to increased risks of myocarditis
Several recent studies have shown an increased prevalence of myocarditis following COVID-19 vaccination.
“Delayed Vigilance: A Comment on Myocarditis in Association with the COVID-19 Injections,” by Karl Jablonowski, Ph.D. and Brian Hooker, Ph.D., P.E., published Oct. 17, 2022 in the International Journal of Vaccine Theory, Practice, and Research, found that two months after COVID-19 vaccines were rolled out to the public, a statistically significant safety signal for myocarditis in males ages 8 to 21 appeared in VAERS.
However, as previously reported by The Defender, even though this safety signal was visible as early as Feb. 19, 2021, CDC officials waited until May 27, 2021 before alerting the public.
By then, over 50% of the eligible U.S. population had received at least one mRNA COVID-19 vaccine — and the FDA expanded the EUA of the Pfizer-BioNTech vaccine to include adolescents 12 and older.
Another study, released April 15, 2022 by seven Israeli researchers, examined the incidence of myocarditis and pericarditis in adults previously were infected with COVID-19, between March 2020 and January 2021.
Despite arguments that an increase in myocarditis diagnoses may be attributed to COVID-19 infections instead of the vaccines, the study “did not observe an increased incidence of either pericarditis nor myocarditis in adult patients recovering from COVID-19 infection.”
As of March 3, 16,641 cases of myocarditis were recorded in VAERS following the receipt of a COVID-19 vaccine or booster — with the number growing to 16,660 when including diagnoses of bacterial myocarditis, infectious myocarditis, mycotic myocarditis, post-infection myocarditis and septic myocarditis.
Of the latter number, 10,701 cases (64.2%) were recorded in males.
While the age of over half of the patients in these recorded cases was listed as “unknown,” in cases where an age was recorded, myocarditis diagnoses peaked in the 18-29 year age group, with high prevalence also found in the 6-17 and 30-39 age groups.
Of 2,778 cases in the 18-29 age group, 2,211 were recorded in males — further indicating the particularly high risk of myocarditis young males face following COVID-19 vaccination.
More governments raising concerns about myocarditis
As early as October 2021, Sweden’s Public Health Agency paused Moderna’s COVID-19 vaccine for people born 1991 and later, “as data pointed to an increase of myocarditis and pericarditis among youths and young adults that had been vaccinated,” according to Reuters.
At around the same time, Finland’s public health authorities also paused the vaccine in young people.
And in November 2022, Sweden paused the Novavax COVID-19 vaccine for those under 30, due to an increased risk of myocarditis and pericarditis.
As reported by The Defender in June 2022, Novavax received EUA from the FDA despite “Multiple events of myocarditis/pericarditis” recorded during clinical trials.
Earlier this week, Yanagase Hirofumi, a member of Japan’s House of Councillors, accused the Japanese government of covering up injuries and deaths stemming from the mRNA COVID-19 vaccines.
Hirofumi told the House of Councillors that in Japan’s vaccine-related adverse events tracking system, at least 2,001 deaths following COVID-19 vaccination have been recorded.
BREAKING
The excess mortality caused by vaccination is making waves in the Japanese Diet.
In Japan, the number of deaths after vaccination has increased by 210,000 since 2020, the highest number since the World War II.
People are dying immediately after vaccination, and… https://t.co/0dDnDtJndfpic.twitter.com/03vB4BYaDR
— You (@You3_JP) March 13, 2023
However, despite “approximately 260 cases in which the doctor in charge reported that there was probably a link between the vaccine and the death” and, citing Japan’s health minister, “52 cases where a pathologist has performed an autopsy, and reported that there is a link between the vaccine and the death,” the database indicates that “only one case has been found to have a causal relationship between the vaccine and death.”
Hirofumi cited the example of “a man in his 30s” who “died three days after receiving the second dose of the vaccine. The cause of death was myocarditis,” adding that “ as a result of the autopsy, doctors concluded that there was a link between the vaccine and the death.”
In an interview on Sunday, Germany’s federal minister of health Karl Lauterbach — previously a proponent of a national vaccine mandate who had stated the COVID-19 vaccines had “no side effects” —admitted that serious adverse events were prevalent and that the vaccine injured are being ignored by the authorities.
The False Messaging about COVID Shots Given to Pregnant Women by Media Liars [Consent to Medical Experiments Obtained by Inducement, Coercion, HalfTruths, Nondisclosures is Fraud, Battery or Murder]
/
From [HERE] The mRNA “vaccines” were released globally in early 2021 with the slogan ‘safe and effective.’ Unusually for a new class of medicine, they were soon recommended by public health authorities for pregnant women.
Recently, a lengthy vaccine evaluation report sponsored by Pfizer and submitted to the Australian regulator (TGA) dated January 2021 was released under a Freedom of Information request.
The report contains significant new information that had been suppressed by the TGA and by Pfizer itself. Much of this relates directly to the issue of safety in pregnancy, and impacts on the fertility of women of child-bearing age:
1. The “vaccine” travels throughout the body after injection, and is found not only at the injection site, but in all organs tested, with high concentration in the ovaries, liver, adrenal glands, and spleen.
Authorities who assured vaccinated people in early 2021 that the vaccine stays in the arm were, as we have known for two years, lying.
2. A doubling of pregnancy loss in the intervention group represents a serious safety signal.
Rather than take this seriously, the authors of the report compared the outcomes to historical data and ignored the outcome because other populations had recorded higher overall losses. This analysis is alarming as remaining below the highest previously recorded pregnancy loss levels in populations elsewhere is not a safe outcome when the intervention is also associated with double the harm of the control group.
3. There were higher rates of fetal malformations in each of the 12 categories studied. Of the 11 categories where Pfizer confirmed the data is correct, there are only 2 total abnormalities in the control group, versus 28 with the mRNA vaccine (BNT162b2). In the category which Pfizer labelled as unreliable, there were 3 abnormalities in the control group and 12 in the vaccinated group.
As with the increased pregnancy losses, Pfizer simply ignored the trend and compared the results with historical data. This is very significant as it is seen across every malformation category. The case control nature of the study design is again ignored, in order to apparently hide the negative outcomes demonstrated.
These data indicate that there is NO basis for saying the vaccine is safe in pregnancy. Concentration of LNPs in ovaries, a doubled pregnancy loss rate, and raised fetal abnormality rate across all measured categories indicates that designating a safe-in-pregnancy label was contrary to available evidence.
The data implies that not only was the Government’s “safe and effective” sloganeering not accurate, it was totally misleading with respect to the safety data available.
[MORE]
COVID Injections Have Killed 50% More People than "COVID" According to a Joel Smalley Analysis
/From [JOEL SMALLEY] Frankly, there’s not much more evidence we can add as proof that pretty much every excess death, health injury and economic woe of the last few years is due to government intervention, ably aided and abetted by the mainstream media and the zombie plebs.
Anyway, whilst waiting for the (Don’t) Care Quality Commission (CQC) to actually provide data in a usable format so that I can lay bare the full extent of carnage visited upon care home residents in England, I approached the Office for Flawed Statistics (ONS) to update the deaths by date of occurrence and age dataset I commissioned. Thy wanted another £360 and 8 weeks… Oh well, I guess a few more people will die unnecessarily because I can’t be bothered if they can’t be bothered.
Struggling for anything really new to report, I thought I would revisit South Korea (mortality data, not the country, unfortunately - not that I’ve ever been but I would like to. There was a nice chap I befriended on LinkedIn in the very early days who said I would always be welcome as his guest - “I miss the smiles”).
So, here is the evidence, and nothing but…

Exhibit 1: there was no unexpected or unusual death in Korea for the first 18 months of the global, ahem, “pandemic” - not until almost the entire country was jabbed at any rate, near enough 100% of the adult population. Weird that.
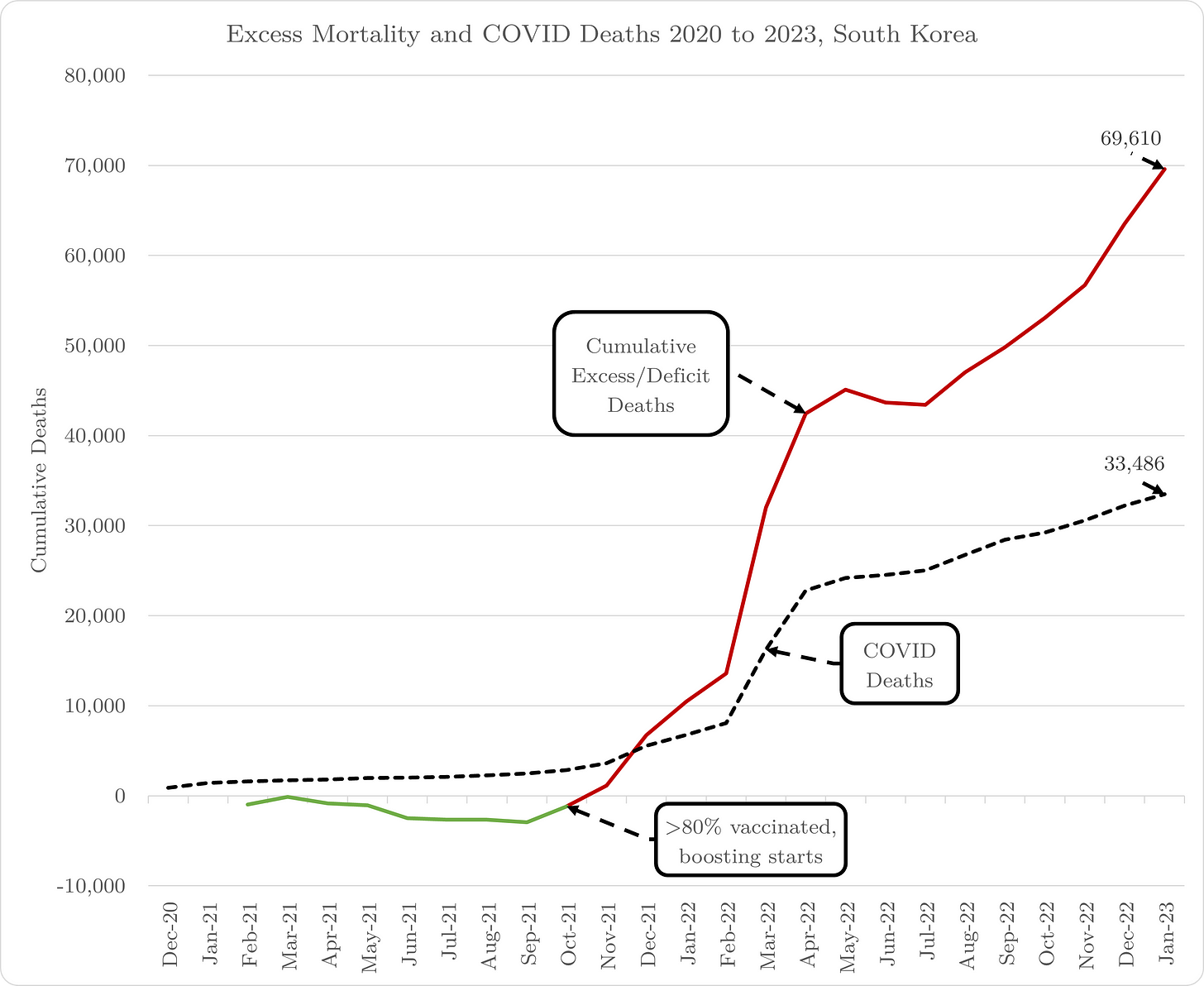
Exhibit 2: as a matter of fact, Korea experienced less mortality than expected for the first 18 months of the “pandemic”, including a rather meagre 3,000 “COVID” deaths. Post-vaccination, excess deaths soared. COVID deaths really took off too but nowhere near as much as overall excess deaths. The most recent data (to Jan-23) shows just over 33,000 COVID deaths and more than twice as many excess deaths at almost 70,000.
Based on the evidence, and a massive dose of logic 1 (and no censorship because I’m not beholden to any indoctrination education establishment or publishing in any controlled “medical” journals, I consider the COVID deaths to be jab deaths, as well as all the other excess deaths - unless you really think that “lockdown” deaths only coincidentally occur after jabs, naturally…).
So, that’s roughly 70,000 jab deaths on a vaccinated population of around 38.7 million. In other words, a jab fatality rate of 0.18% which is pretty consistent with quite a few other studies, including the infamous Skidmore one retracted involuntarily.
If we extrapolate that across the whole “vaccinated” world (5.57 billion according to OWID), I estimate just over 10 million people have been killed by the jab. That compares to 6.9 million “COVID” deaths (which includes a whole load that are actually jab deaths as I have set out above 2), i.e. at least 150%.
I know it’s a collective effort but that would put all the world “leaders” who sanctioned the democide in their countries at 4th spot in the table of most murderous dictators, behind Hitler (17 million), Stalin (23 million) and Mao Zedong (50+ million).
The difference is that most people don’t even realise…1
The logic being that after 18 months, for Korea to experience such a massive increase in “COVID” deaths implies that either the virus became more virulent or the host (that's us humans) became more vulnerable. Despite not being an epidemiologist or a virologist, I have spent rather a lot of time in the last few years with decent scientists across the spectrum and no-one can provide me credible evidence of a respiratory pathogen mutating to become more virulent. Conversely, I've personally read several dozen papers and articles setting out myriad modes of action on the part of the novel mRNA product subverting the immune system. And you know what a fan I am of Occam's razor?! 2
If you accept the jab-induced COVID hypothesis, it's not unreasonable to remove around 3 million of these deaths from the COVID side.
Gov Data (VAERS) COVID Shows Shots have Caused 1,544,510 Adverse Events (288,607 Serious Injuries and 35,096 Deaths) VAERS Under Reports by a Factor of 4 to 5 times, w/an Accuracy Rate as Low as 1%
/
From [HERE] Data published Friday by the Vaccine Adverse Event Reporting System (VAERS) show 1,544,510 adverse events following COVID-19 vaccines were reported between Dec. 14, 2020, and April 7, 2023. This includes 288,607 reports of serious injuries and 35,096 deaths.
Of the 35,096 reported deaths, 21,905 cases are attributed to Pfizer, 9,920 to Moderna, 2,995 to Johnson & Johnson, and 18 to Novavax. Of the reported deaths, 9% occurred within 24 hours of vaccination, and 13% occurred within 48 hours.
VAERS is a voluntary reporting system co-managed by the U.S. Food and Drug Administration and Centers for Disease Control and Prevention (CDC) designed to detect vaccine safety signals.
In the U.S., 673 million COVID-19 vaccine doses had been administered as of March 27, including 401 million doses of Pfizer, 252 million doses of Moderna, 19 million doses of Johnson & Johnson, and 82,000 doses of Novavax.
Bivalent Booster Data
As of April 12, the CDC reported 55.5 million people had received an experimental bivalent booster dose targeting the no-longer-existing Wuhan strain and obsolete BA.4/BA.5 omicron subvariants.
Since the rollout of bivalent boosters in September 2022 and April 7, there have been 28,141 adverse events reported to VAERS, with 40% attributed to Moderna’s booster and 60% attributed to Pfizer/BioNTech. The data included 240 deaths, 2,187 serious injuries, and 80 reports of myocarditis and pericarditis (heart inflammation).
The CDC uses a narrowed case definition of myocarditis. To meet the case definition of myocarditis, people must have had “symptoms such as chest pain, shortness of breath and feelings of having a fast-beating, fluttering or pounding heart, and medical tests to support the diagnosis of myocarditis and rule out other causes.” This allows them to exclude cases of cardiac arrest, ischemic strokes, and deaths due to heart problems that occur before one has the chance to go to the hospital, obtain a diagnosis, or “dies suddenly.”
The CDC website does not state what happens to these cases, but there is no indication they are tracked or included in the CDC’s myocarditis numbers.
Data for 6-month-olds to 5-year-olds
6,122 adverse events, including 264 cases rated as serious and 14 reported deaths.
5 reports of myocarditis and pericarditis.
36 reports of blood clotting disorders, which means the CDC throttled at least 12 reports of blood clotting over the previous week.
61 reports of seizures.
Data for 5- to 11-year-olds
17,298 adverse events, including 840 rated as serious and 34 reported deaths.
48 reports of myocarditis and pericarditis.
76 reports of blood clotting disorders.
195 reports of seizures.
Data for 12- to 17-year-olds
41,692 adverse events, including 4,683 rated as serious and 140 reported deaths.
276 reports of anaphylaxis among 12- to 17-year-olds where the reaction was life-threatening, required treatment, or resulted in death.
1,357 reports of myocarditis and pericarditis, with 1,187 cases attributed to Pfizer’s vaccine.
313 reports of blood clotting disorders, with 285 cases attributed to Pfizer.
33 cases of postural orthostatic tachycardia syndrome (POTS) were attributed to Pfizer’s vaccine.
Data for all age groups to VAERS
16% of deaths were related to cardiac disorders.
53% of those who died were male, and 41% were female. The remaining death reports do not list the gender of the deceased.
The average age of death was 72.
As of April 7, 9,085 pregnant women reported adverse events related to COVID-19 vaccines, including 5,259 reports of miscarriage or premature birth.
Of the 17,209 cases of Bell’s palsy reported, 73% were attributed to Pfizer vaccinations, 22% to Moderna, and 5% to J&J.
3,293 reports of Guillain-Barré syndrome.
10,420 reports of anaphylaxis where the reaction was life-threatening, required treatment or resulted in death.
8,580 reports of myocardial infarction and cardiac arrest.
46,538 reports of blood-clotting disorders. Of those, 31,967 reports were attributed to Pfizer, 10,510 reports to Moderna, and 3,985 reports to Johnson & Johnson.
25,621 cases of myocarditis and pericarditis, with 19,461 cases attributed to Pfizer, 5,643 cases to Moderna, and 454 to Johnson & Johnson.
83 cases of Creutzfeldt-Jakob disease, with 67 cases attributed to Pfizer, 15 to Moderna, and 2 to J&J.
727 cases of POTS, with 538 cases attributed to Pfizer, 158 cases to Moderna, and 30 cases to Johnson & Johnson.
Although healthcare providers are required by law to report vaccine adverse events to VAERS, research shows very few do. It is essential that anyone who experiences an adverse event report their own injury.
Documents Reveal the US Government Incentivized Coin-Operated Doctors to Inject Medicaid Patients w/Experimental, Deadly COVID Shots by Offering Bonuses Based on the Number Successfully “vaccinated"
/From [HERE] The federal government and insurers incentivized healthcare providers in Kentucky and California to vaccinate Medicaid patients against COVID-19 by offering bonuses based on the percentage of patients successfully vaccinated.
“[This is] truly sickening and I am embarrassed for my profession by this,” Dr. Meryl Nass, an internist and biological warfare epidemiologist, wrote on her Substack, where she posted several documents relating to the COVID-19 vaccine provider incentive programs.
The documents help to draw a picture of the broader effort at the federal, state and local levels to unleash a range of strategies targeting low-income and people-of-color communities, which tended to have lower vaccination rates.
The strategies included providing hundreds of millions of dollars for the creation of “culturally tailored” pro-vaccine materials and for training “trusted” and “influential messengers” to promote COVID-19 and flu vaccines to communities of color in every state.
Nass’ revelations showed these efforts went beyond advertising, fear campaigns, payments to patients and payments to trusted community actors and included, in some cases, direct financial incentives to healthcare providers.
Kentucky: Medicaid paid doctors up to $250 per vaccinated Medicaid patient
Anthem Blue Cross and Blue Shield Medicaid in Kentucky told physicians in 2021 it would “recognize your hard work by offering incentives for helping patients make the choice to become vaccinated.”
The more people vaccinated, the higher the per-person incentive.
For physicians who treated an Anthem Medicaid cohort with a minimum of 25 patients in their practice, Anthem Medicaid offered incentives for vaccination by Sept. 1, 2021, that ranged from a $20 bonus per vaccinated person for physicians who vaccinated 30% of the cohort, to $125 per vaccinated person for those who vaccinated 75% of the cohort, with several incremental steps in between.
As time went on, the rates increased.
Between Sept. 1 to Dec. 31, 2021, physicians received payments ranging from $100 per newly vaccinated person for those who vaccinated 30% of their patient cohort, to $250 per newly vaccinated person for those who vaccinated 75% of their patient cohort.
In 2022, the Anthem provider incentive program changed to a flat rate. Providers received $50 per newly vaccinated Medicaid patient. This included children ages 6 months to 4 years and kids 12 and older vaccinated between Jan. 1 and Dec. 31, 2022, and children ages 5 to 11 vaccinated between June 1 and Dec. 31, 2022.
Medi-Cal: $350 million in incentives to vaccinate low-income children, people of color
The California Department of Health Care Services (DHCS) on Aug. 6, 2021, announced $350 million in incentive payments — $250 million to providers and $100 million for direct non-monetary payments, such as gift cards, to vaccine recipients — to encourage vaccination among Medi-Cal’s 14 million beneficiaries.
Of the $350 million, $175 million came from state general funds and $175 million from federal funding. The funding period lasted from Sept. 2, 2021, through Feb. 29, 2022.
The program offered incentives to managed care plans in the name of “health equity.” In the press release, DHCS Director Will Lightborne said that raising rates among Medi-Cal beneficiaries was essential because “California will only be safe when everyone is safe.”
Nass noted that this program was rolled out one day after Centers for Disease Control and Prevention Director Rochelle Walensky told CNN the vaccines don’t prevent virus transmission. “That’s clearly a contradiction,” Nass told The Defender.
The funding targeted Medicaid recipients with low vaccine uptake — the homebound, communities of color, youth ages 12 to 25 and people ages 50 to 64 with multiple chronic conditions — and incentivized outreach and vaccination activities for providers and pharmacies.
At the time of the announcement, only 45.6% of Medi-Cal beneficiaries age 12 and over had received at least one dose of the COVID-19 vaccine, compared to over 76% of Californians overall.
The DHCS funding included payments to community-based organizations, food banks, advocacy groups and faith-based organizations. This key strategy of funding grassroots leaders to act as “grassroots” proxies spreading the federal government’s vaccine message was widespread throughout the pandemic.
Providers could also couple this grant with a CAIRVaxGrant, which offered providers up to $10,000 to enter all of their historical electronic health record immunizations into the California Immunization Registry (CAIR).
The grant stipulated that after startup costs, payments would be directly tied to “meeting specific vaccination goals,” similar to the Kentucky program.
The incentive payment structure under the California plan was complex, paying a financial reward to healthcare providers who met particular benchmarks that varied by county and demographic but overall increased the percentage of vaccinated patients among their Medicare beneficiaries.
Under this incentive structure, providers had to meet particular vaccination targets in order to get paid. Those who were especially successful in increasing vaccination rates in the target groups would be entered into a “high performance pool,” receiving extra money for substantially moving the vaccination rates for Medicaid recipients 75% higher than baseline or within 10% of a given county’s general rate.
In the equation that determined the incentive payment structure, different demographic groups were weighted differently. For example, vaccine recipients ages 12 to 25 were weighted more highly than older recipients and those in the two racial/ethnic groups with the lowest uptake were also given greater weight.
By Jan. 21 of this year, despite this $250 million push, Medi-Cal vaccination had only increased to 52.9%.
Medicaid pays doctors more to administer COVID vaccines than other shots
As part of the American Rescue Plan Act, the Biden administration fully funded the COVID-19 vaccination program, making vaccines free regardless of health insurance status.
To cover the costs of the uninsured and underinsured, the Health Resources and Services Administration (HRSA) paid provider costs of vaccine administration through an Uninsured Program and a COVID-19 Coverage Assistance Fund.
Reimbursements were based on national Medicare rates, but the Centers for Medicare & Medicaid Services (CMS), which sets those rates, increased the reimbursement rate over time. Through March 14, 2021, HRSA paid $28.93 for a single-dose vaccine or for the second dose in a series of 2, and $16.94 for the first dose in a series of two.
On March 15, 2021, those rates increased to $40 per dose and $75.50 for an “in-home” dose of the vaccine.
Nass said the initial payments were in line with Medicaid payments for other vaccines, but the increased payment marked a departure from the usual reimbursement structure.
Usually, all CMS changes to Medicare payments for specific services must go through notice and comment rulemaking, but “to save time during the COVID-19 pandemic, the agency bypassed that route before increasing payments for administering the vaccines,” JAMA reported.
CMS said the higher payments were meant to help expand COVID-19 vaccination, supporting “actions taken by providers, such as growing existing vaccination sites, conducting patient outreach and education, and hiring additional staff,” Healthcare Finance News reported.
CHD Sues NIH Over Failure to Comply With FOIA Request for Correspondence With COVID Shot Injury Victims
/From [HERE] Children’s Health Defense (CHD) on Wednesday sued the National Institutes of Health (NIH) for failing to respond to CHD’s Freedom of Information Act (FOIA) request for documents related to correspondence between NIH researchers and individuals who contacted the NIH regarding adverse events they experienced after receiving the COVID-19 vaccine.
According to the complaint, filed in the U.S. District Court for the District of Columbia, CHD submitted the FOIA request Nov. 10, 2022. The NIH has not produced the documents or a final determination and stopped responding to CHD.
CHD alleges the NIH violated the legal time limits for responding to FOIA requests and is withholding crucial information from the public.
“Lawsuits like this are critically important,” said Kim Mack Rosenberg, CHD acting general counsel. “Government transparency concerning its research on injuries following COVID-19 injections is of paramount importance.”
Rosenberg added:
“The U.S. government has encouraged, and in some cases, mandated, these injections. How can it now turn a blind eye to requests for information concerning injuries?
“Individuals have a right to this information to promote informed decision-making. By ignoring CHD’s FOIA request, NIH only further undermines the public’s trust in NIH and other government agencies.”
Several vaccine injury victims who communicated with the NIH spoke to The Defender about their experiences interacting with the NIH and participating in a study it was conducting on vaccine-injured individuals — although the NIH has since, on several occasions, denied having data on such individuals or even conducting such research. [MORE]
[Government is Trying to Kill You] 45 Times as Many Deaths After COVID Shots in Just 2 Years Compared With All Flu Vaccine-Related Deaths Since 1990, Data Show
/From [CHD] The cost of injecting healthy people, “especially children,” with a Pfizer or Moderna COVID-19 vaccine “outweighs any claimed though unvalidated benefits,” according to researchers who analyzed adverse events data from more than 10 regulatory surveillance and self-reporting systems during the first two years of the COVID-19 vaccine rollout.
“Our meta-analysis of both national and international vaccine adverse events emphasizes the importance of re-evaluating public health policies that promote universal mass injection and multiple boosters for all demographic groups,” said the authors of a peer-reviewed studypublished this month in the International Journal of Vaccine Theory, Practice, and Research.
Eliana Romero, Ph.D., director of clinical research at the Neurodiversity Foundation, Shawn Fry, founder and chief science officer of the Neurodiversity Foundation and Brian Hooker, Ph.D., P.E., chief scientific officer of Children’s Health Defense and associate professor of biology at Simpson University in Redding, California, authored the paper.
The researchers looked at adverse events specifically related to cardiovascular and fertility health — such as myocarditis and menstrual abnormalities — that went overlooked during the “expedited safety analyses” that took place in the “accelerated approval process that allowed the manufacturers to fast-track their products,” they said.
They analyzed data from the Vaccine Adverse Event Reporting System (VAERS) database — the primary government-funded system for reporting adverse vaccine reactions in the U.S., which has been shown to report only 1% of actual vaccine adverse events — and the Defense Medical Epidemiology Database (DMED), the medical events database for all active and reserve U.S. military.
The authors also examined data from other regulatory surveillance and self-reporting systems including the V-safe After Vaccination Health Checker, the U.K.’s Yellow Card reporting system, Public Health Scotland, the Israeli Ministry of Health and the Natural Cycles App.
Hooker said the data highlights “the dramatic uptick in adverse events associated with the COVID-19 vaccine.”
After carefully conducting statistical analyses, the authors concluded there were far more reports of adverse events following COVID-19 vaccination than following either influenza or pertussis vaccination.
The researchers also found “statistically significant higher numbers of hospital encounters in military personnel” after the COVID-19 vaccine rollout when compared to just before the rollout, and “increases in incidences of thromboembolic conditions, such as menstrual abnormalities, myocarditis, and cerebrovascular events after the implementation of COVID injection mandates, compared to the preceding five years.”
The researchers verified their conclusions by comparing their findings to similar reports from other regulatory surveillance and self-reporting systems including EudraVigilance, Eurostat, German health insurers and the U.K.’s Office for National Statistics.
In addition to statistically significant increases in vaccine adverse events, the data showed “highly statistically significant” increases in “specific morbidity” and “all-cause mortality,” Hooker told The Defender.
“These results should not be ignored,” he added.
More than 45 times as many deaths after COVID shots than all flu vaccine deaths combined since 1990
The researchers found the number of reported deaths related to an mRNA COVID-19 vaccine was more than 45 times as many deaths per vaccine dose as were reported for all the influenza vaccines combined since 1990.
They also found a higher incidence of menstruation problems, myocarditis and cerebrovascular events following COVID-19 vaccination than following influenza vaccination, as seen in figure 1A:

The researchers also compared adverse events reported in VAERS following the COVID-19 vaccines to adverse events reported following the influenza and pertussis vaccines.
They showed the percentage of total reports attributed to death, for the COVID-19, influenza and pertussis vaccines, as seen in figure 1B:

Should the trends in myocarditis rates continue, “we will see spikes in death rates attributed to the increase in myocarditis documented above, as well as in the number of otherwise healthy young adults needing transplants to survive, and all the complications associated with such a transplant,” the authors said.
DMED data trends mirrored VAERS and other surveillance data trends, which showed dramatic increases in many medical conditions in 2021 after the COVID-19 vaccine rollout when compared to the previous five years.
The researchers also pointed out that on Feb. 1, 2022, Sen. Ron Johnson (R-Wis.) wrote a letter to U.S. Secretary of Defense Lloyd J. Austin III asking if the U.S. Department of Defense (DOD) was aware of the DMED data.
“If so,” Johnson said in his letter, “please explain what actions DOD has taken to investigate the root cause for the increases in these diagnoses.”
COVID vaccines not as ‘benign’ as the media said they were
Romero, the paper’s lead author, said the research wasn’t done “for a cause” or “with any predetermined hope for any specific results.”
Romero said she initially “had no qualms” about taking the COVID-19 vaccine, but soon it became “impossible not to hear all the opposition to them and, always a researcher at heart, I decided to follow up.”
Romero holds a doctorate in molecular and human genetics and has worked with some of the world’s top neurogeneticists.
“I’m a scientist through and through,” Romero told The Defender. “I also have Asperger’s, so I’m not exactly wired to tell anything but the truth.”
Romero began finding “mounting evidence the vaccines weren’t as benign as the media was desperately trying to convince us they were,” she said and felt an obligation to share what she was finding with others.
Romero — who has 20 years of experience investigating the genetic and biological aspects of various disease states at Baylor College of Medicine, Children’s Hospital of Pennsylvania, Johns Hopkins University and several private laboratories — said she used “all avenues available” and “went through every effort to standardize my data, compare apples to apples, and to perform any calculations I knew of to test the validity of the data presented.”
“The paper isn’t an attempt to skew anybody’s opinions one way or the other,” Romero emphasized. “Its sole purpose is to make sure people have all the information they need to make the best decisions they can for their health,” she said.
“Governments and institutions and scientists and doctors should provide people ALL the information needed so that individuals can make truly informed decisions for themselves.”
Are You Eating Pork Injected With Merck’s mRNA Livestock Vaccine?
/Story at a glance:
For the last couple of years, I’ve recommended not eating pork due to its high linoleic acid (LA) content, but there’s an even bigger reason to avoid it now. Since 2018, pork producers have been using customizable mRNA-based “vaccines” on their herds.
The very first RNA-based livestock vaccine, a swine influenza (H3N2) RNA shot licensed in 2012, was developed by Harrisvaccines. The company followed up with an avian influenza mRNA shot in 2015. Harrisvaccines was acquired by Merck Animal Health later that year.
CureVac developed an mRNA-based rabies shot for pigs in 2016.
The swine vaccine platform Sequivity, introduced in 2018, was developed by Merck in partnership with Moderna. Sequivity can produce endlessly customized “vaccines,” none of which undergo safety testing.
Americans have been eating pork treated with gene therapy for nearly five years already, and even more of our meat supply is about to get the same treatment. mRNA-lipid nanoparticle shots for avian influenza are in the works, as are mRNA shots for cows. Lobbyists for the Cattlemen’s Association recently confirmed they intend to use mRNA “vaccines” in cattle, which might affect both dairy and beef.
Missouri House Bill 1169 would require labeling of products that can alter your genes. It would also require companies to share information about the potential transmissibility of gene-altering interventions, and asserts that fully informed consent must be given for all vaccines, gene therapies and medical interventions.
From [HERE] For the last couple of years, I’ve recommended not eating pork due to its high linoleic acid (LA) content, but there’s an even bigger reason to avoid it now.
Since 2018, pork producers have been using customizable mRNA-based “vaccines” on their herds, and this has slipped completely under the radar. I myself just found out about it.
As described on Merck’s animal health website:
“A revolutionary swine vaccine platform, SEQUIVITY harnesses RNA particle technology to create customized prescription vaccines against strains of influenza A virus in swine, porcine circovirus (PCV), rotavirus and beyond. It’s supported by a sophisticated dashboard filled with comprehensive data and insights …
“Sequivity is a custom swine vaccine platform … Sequivity only targets swine pathogen gene sequences of interest. Doesn’t replicate or cause disease, delivering pathogen information to the immune system … There’s no need to transfer or handle live material like autogenous, killed or modified live vaccines …
“Targets existing and evolving swine pathogens, including diseases not covered by conventional swine vaccines. Allows for the creation of multivalent formulations by blending RNA particles to target multiple swine pathogens in one shot.”
First RNA ‘vaccine’ for livestock licensed in 2012
Merck was not alone in developing veterinary mRNA shots, however. They weren’t even first on the scene, although they later acquired the company that started it all.
The very first RNA-based livestock vaccine, a swine influenza (H3N2) RNA shot, was licensed over a decade ago in 2012, and was developed by Harrisvaccines. The company followed up with an avian influenza mRNA shot in 2015. Harrisvaccines was acquired by Merck Animal Health later that year.
CureVac developed an mRNA-based rabies shot for pigs in 2016. (On a side note, they began conducting human rabies shot trials in 2020 in response to the World Health Organization’s goal to achieve “zero human rabies deaths by 2030.”)
In 2016, Bayer also partnered with BioNTech to develop mRNA “vaccines” for both livestock and pets, but it doesn’t appear they ever launched anything.
So, in retrospect, it appears Americans have been eating pork treated with gene therapy for the past five years, and even more of our meat supply is about to get contaminated with the same treatment.
In addition to the avian influenza RNA shot for chickens licensed in 2015, newer mRNA-lipid nanoparticle shots for avian influenza are also in the works.
Iowa State University is also working on an mRNA shot for cows, and lobbyists for the Cattlemen’s Association recently confirmed they intend to use mRNA “vaccines” in cattle, which might affect both dairy and beef.
Merck and Moderna: Partners in mRNA jab race since 2015
The same year Merck purchased Harrisvaccines (2015), it also entered into a partnership with Moderna to develop a number of undisclosed mRNA “vaccines.” It was slated to be a three-year collaboration, with a one-year optional extension, in which Merck would perform research and development and commercialization of five potential products using Moderna’s mRNA technology.
As reported by Genetic Engineering & Biotechnology News at the time:
“Moderna has agreed to design and synthesize the mRNA product candidates directed against selected targets through its mRNA Therapeutics™ platform.
“The platform builds on the discovery that modified mRNA can direct the body’s cellular machinery to produce nearly any protein of interest — ranging from native proteins to antibodies and other entirely novel protein constructs with therapeutic activity inside and outside of cells.”
Endless customization, zero safety testing
Sequivity, introduced in 2018, was one of the products that came out of that partnership. As explained by Merck (both on its website and in the video below), Sequivity is not so much a single vaccine as it is a platform that can be endlessly customized — all without additional safety analyses over and beyond the initial ridiculously inadequate testing.
As noted by Zoetis, the largest producer of veterinary drugs and vaccines:
“Sequivity has safety and efficacy studies based on the platform with a historical initial isolate, not likely the isolate that customers would be requesting in their product.”
Sequivity is customized as follows:
Pathogen is collected and sent to a diagnostic lab.
The gene of interest is sequenced and sent electronically to Sequivity analysts.
A synthetic version of the gene of interest is synthesized and inserted into the RNA production platform.
The RNA particles released from incubated production cells are harvested and formulated into a customized “vaccine.”
Using this platform, a customized “vaccine” can be created in as little as eight weeks. Now, what could go wrong by not testing every new shot for safety? [MORE]
A Study by a Leading Expert in Sequencing Methods for DNA and RNA finds that COVID mRNA Shots Contain Excessive Quantities of Bacterial DNA that Cause Severe Health Risks
/by Michael Palmer, MD and Jonathan Gilthorpe, PhD
From [HERE] Recent studies by Kevin McKernan, a leading expert in sequencing methods for DNA and RNA, have revealed that batches of the modified mRNA vaccines produced by both Pfizer and Moderna contain a high proportion of contaminating bacterial DNA. In all, the DNA accounts for up to 20-35% of the nucleic acids contained in each of the vaccine batches. These alarmingly high concentrations far exceed the levels deemed safe by standard-setting organizations such as the European Medicines Agency (EMA). This document summarizes the evidence of that DNA contamination and discusses what possible health risks it implies to the recipients of the vaccines.
1. The role of DNA in the manufacture of mRNA vaccines
1.1. General background
Most readers will be aware that
the synthetic RNAs contained in the COVID-19 mRNA vaccines encode the SARS-CoV-2 spike protein;
in living mammalian cells, the instructions for building a given protein molecule are stored as a gene within the DNA inside the nucleus;
to build a given protein molecule, the cell first transcribes its gene into RNA and modifies the two ends of this molecule to form messenger RNA (mRNA). The mRNA is then transported from the nucleus to the cytoplasm, where it induces the cell’s protein factories—the ribosomes—to translate the mRNA’s nucleotide sequence into the corresponding amino acid sequence and assemble the protein.
1.2. Steps in the manufacture of mRNA vaccines
Since the spike protein is a large molecule, so is the mRNA which encodes it. The total chemical synthesis of large mRNA molecules is not practical at scale. Therefore, in order to obtain the mRNA molecule encoding spike, the process by which cells produce their own mRNAs is mimicked in vitro. This involves the following steps:
A DNA copy of the gene for the spike protein is inserted into a bacterial plasmid. This is a ring-shaped, double-stranded DNA molecule which can exist in a bacterial cell independently of the cell’s own chromosomal DNA, and which can also be copied and passed on to both daughter cells when that cell divides.
The recombinant (artificial) plasmid carrying the spike protein gene is introduced into a cell of the bacterial species Escherichia coli (E. coli ). Since E. coli cells divide very rapidly, this one cell can within a short time be grown up to a very large number of cells. Each of these progeny cells will contain their own inherited copies of the plasmid, and therefore of the spike protein gene.While there is a certain chance of the plasmid being lost from some of the offspring during successive cell divisions, we can enforce its maintenance by giving it a selectable marker, which ensures that only those cells which retain the plasmid will survive. With the plasmids used by both Pfizer and Moderna, this selection marker is a gene which endows the host cells with resistance to the antibiotic kanamycin. To apply the selection, the bacteria are simply grown in the presence of kanamycin.
After growing up a sufficient number of bacterial cells in a nutrient broth containing kanamycin, these cells are broken up and the plasmid DNA is purified from the other bacterial cell components.
The ring-shaped plasmid molecules are converted to linear form using a restriction enzyme, which cleaves both strands of the DNA molecule at a specific, unique site which is located downstream of the spike protein gene. This step is needed to prevent the formation of RNA molecules that are overly long and might have undesired effects in vivo.The linearized DNA molecules can be purified from remaining circular ones, but in what manner and how efficiently this may be done in the production of Pfizer’s and Moderna’s vaccines is not public knowledge.
An RNA polymerase is used, in the presence of the necessary nucleoside building blocks and cofactors, to copy the spike protein gene from the DNA version on the linearized plasmid into the mRNA version. Both Pfizer and Moderna employ the T7 RNA polymerase, which is derived from the eponymous bacteriophage. This enzyme binds to a cognate promotersequence likewise derived from T7 that has been engineered into the plasmid upstream of the gene for the spike protein. This interaction between polymerase and promoter initiates the transcription.At this stage, the synthetic nucleoside N-methyl-pseudouridine (mψU) is incorporated into the artificial RNA instead of the natural uridine nucleoside. When delivered in the form of a vaccine, RNA modified in this manner is less stimulatory to the innate immune system than is RNA containing the natural uridine. It is also more efficiently translated into protein, and under certain conditions more resistant to degradation [1]. Both Pfizer’s and Moderna’s mRNA vaccines contain mψU instead of uridine.
The two ends of each RNA molecule are coupled enzymatically to certain moieties that are also found at these positions within natural mammalian mRNAs, and which enhance its biological activity and stability in vivo.
This steps provide a functional mRNA which is capable of instructing the cells’ ribosomes to produce the spike protein. However, at this stage the product is not yet pure—all of the bacterially derived template DNA is still present. The latter should not be included in the final drug product, because it poses health risks to the recipients (see Section 4). To get rid of this DNA, another enzyme called DNase is added. This should break up the DNA into smaller fragments, which can then be removed from the much larger RNA molecules by filtration and other purification techniques. In the final step, the mRNA is combined with a lipid mixture in order to package it into lipid nanoparticles (LNPs), which induce human cells to take up the mRNA molecule and to make the spike protein.
2. What did we know previously about the DNA contamination problem?
In a nutshell, very little. The FDA’s assessment reports on both vaccines [2,3] do not mention the issue at all. The European Medicines Agency (EMA) assessment report on the Pfizer vaccine mentions that “The robustness of the DNase digestion step is not considered comprehensively demonstrated” [4, p. 17]. Similar language is used in the EMA report on the Moderna vaccine [5, p. 19f]. However, based on this sparse information alone, it is impossible to say whether the problem was considered serious, and what remedies were required by the regulator, if any.
3. Independent evidence about DNA contamination of mRNA products
As of April 3, 2023, Kevin McKernan has described his recent findings in three articles on his Substack site [6–8]. The experiments described in the first two reports were carried out on samples of newly introduced “bivalent” vaccines from Pfizer and Moderna. These preparations resemble the previous “monovalent” ones in their chemical composition, i.e. they should contain highly pure mRNA, complexed with a mixture of lipid (fat-like) molecules into mRNA /lipid nanoparticles. The only difference between the two varieties is that the bivalent vaccines contain a mixture of two mRNAs encoding two antigenic variants of the spike protein. This has no bearing on the technical problem of DNA contamination as such. We note, however, that the extent of DNA contamination may vary between production batches, and that only a small number of batches has so far been characterized in this regard.
3.1. McKernan’s first report
In an initial study [6], McKernan characterized both the RNA and the DNA contained in the mRNA vaccines.
3.1.1. Extraction and direct characterization of nucleic acids from the vaccines
The first step consisted in stripping away the lipids in order to obtain the pure nucleic acids. The solvent-based method that he used does not discriminate between DNA and RNA—if both are present, both will be recovered. The extracted nucleic acids were separated according to size. This revealed not only the expected regular, full-length spike mRNA species, but also smaller fragments, which had been noted previously both by the regulators and in work published by one of the manufacturers [9]. More surprisingly, RNA species larger than the full-length mRNA were also found. These species remain uncharacterized.
3.1.2. Amplification of the extracted nucleic acids
As a preparatory step for determining the exact nucleotide sequences of the extracted nucleic acids, they were amplified by PCR methods. In the case of the RNA, PCR was preceded by reverse transcription into DNA using a dedicated enzyme (reverse transcriptase). Since this study’s primary goal was to study the RNA rather than the DNA, this amplification step was biased against DNA through the addition of actinomycin D, which under the given experimental conditions selectively inhibits DNA synthesis. Accordingly, relatively low amounts of DNA were recovered in the amplified sample. Nevertheless, in case of the Pfizer vaccine, the amount of DNA determined to be present already exceeded EMA’s arbitrarily decided limit for the maximal permissible proportion of DNA per RNA.
3.1.3. DNA sequencing results
With both Pfizer’s and Moderna’s products, DNA sequences of complete DNA plasmids were obtained, although some ambiguity remained in the case of the Moderna plasmids. The features of the plasmid sequences will therefore be discussed in connection with McKernan’s second study, which used more and more pure DNA for sequencing and therefore provided more reliable results.
3.2. McKernan’s second report
The second study [7] focused on quantifying and characterizing the DNA contamination that was qualitatively detected in the first one.
3.2.1. Plasmid DNA contained in the mRNA vaccines is competent to propagate in bacterial cells
In the first experiment, it was determined whether the plasmid DNA whose presence had been inferred from the previous sequencing results is indeed biologically functional, to the extent that it can be introduced into and persist within bacterial cells. To this end, nucleic acids were again extracted from the vaccine samples. These nucleic acids were mixed with a suspension of E. coli cells that had been rendered competent for DNA uptake.
After inducing these cells to take up the DNA and giving them some time to recover, they were spread onto Petri dishes filled with solidified growth medium containing kanamycin. As noted earlier, kanamycin will kill any E. coli cells that do not contain a resistance gene to it. Therefore, the observed growth of bacterial colonies on those Petri dishes confirmed that some cells had indeed acquired resistance to kanamycin by taking up and propagating the plasmids. This was observed with both the Pfizer and the Moderna vaccine samples.
In this context, we should note that only circular plasmid molecules, but not linearized ones, can be efficiently introduced into bacterial cells. The success of this experiment therefore suggests that some of the plasmid molecules had escaped the linearization step (step 4 in Section 1.2) and made it all the way through the production process in the circular form which exists in bacterial cells. On the other hand, since the number of bacterial colonies observed in this experiment was not high, it is likely that most of the DNA had indeed been linearized. Because the biological hazards of foreign DNA within our own body may vary depending on whether it is linear or circular, the likely presence of both forms in the vaccines is worth noting. The exact proportions of circular and linear DNA in the mixtures remain to be determined.
3.2.2. The abundance of contaminating DNA
The second major finding of this study is the quantitation by PCR of both DNA and mRNA contained in the vaccine samples. As you may be aware, in a PCR reaction, a chosen segment of a nucleic acid sequence is reduplicated by enzymatic synthesis in several successive reaction cycles. From the number of cycles (or doublings) necessary to reach a certain threshold concentration, we can calculate how many copies of the target sequence were present at the outset.
In these experiments, the chosen experimental format was multiplex PCR, i.e. two target sequences were amplified in a single reaction mixture. One of these targets was within the spike protein gene, and it thus should be present both on the plasmid DNA molecules and on the spike mRNA molecules transcribed from them. In order to include the mRNA molecules in this amplification, PCR was again preceded by reverse transcription.
The other target sequence was within the kanamycin resistance gene, which should be present only on the plasmid DNA. By comparing the number of cycles required for each of the two targets to cross the threshold, it was determined that up to 35% of the total nucleic acid contained in the vaccines is in fact DNA. For comparison, the EMA has stipulated that DNA should not amount to more than 0.033% of the total nucleic acids.
3.2.3. Determination of plasmid DNA sequences
The plasmids that had originally been contained in the vaccines and then been introduced into bacterial cells (see Section 3.2.1) were again isolated from those bacterial cultures, and their complete DNA sequences were determined. Such sequences were provided in full in McKernan’s first study [6], but he indicated that he was still working on corroborating and refining the sequencing data. Meanwhile, the functional features of the plasmid DNA found in the Pfizer vaccine samples are shown in Figure 1. They will be discussed in connection with the risk assessment.






































































































































































































































































