Fingerprints of NYC Teachers Who Refused to Get COVID Injections Sent to FBI, Affidavit Says
/From [HERE] Unvaccinated New York City teachers were reportedly “flagged” and their fingerprints sent to the FBI, according to an affidavit filed in federal court last week.
In the New Yorkers for Religious Liberty Inc. v. The City of New York appeals hearing, challenging the now-rescinded vaccine mandate for city employees, plaintiff’s attorney John Burch said that “flagged” teachers were labeled with “problem codes” that impact their ability to get another job.
The allegations were based on a June 2022 affidavit written by Betsy Combier, president of the due process advocacy group Advocatz, detailing how the New York City Department of Education (DOE) flagged unvaccinated teachers without evidence of misconduct and sent their information, including fingerprints “to the national databases at both the Federal Bureau of Investigation and [New York’s] State Division of Criminal Justice Services.”
Sujata Gibson, an attorney representing the plaintiffs, commented on these revelations to The Defender:
“These are hardworking teachers and educators with excellent employment records who dedicated their lives to teaching in the New York City public schools. It is unacceptable that the DOE would place problem codes on their employment files and flag their fingerprints with the FBI simply because they were not able or willing to get vaccinated.
“This was never about public health. This was about punishing those whose religious and other beliefs don’t line up with corporate interests in an effort to make it impossible to dissent.”
Michael Kane, national grassroots organizer for Children’s Health Defense and founder of Teachers For Choice, reported the “problem codes” on Feb. 9, one day after the hearing in the 2nd U.S. Circuit Court of Appeals.
He explained the relevance of this information for the case to The Defender:
“The point our attorneys were making is that not only were our constitutional rights violated when the mandates first occurred, but that these violations continue to occur, because this problem code is put on for us practicing our sincerely held religious beliefs. And when we go to apply for jobs, it’s still blocking us.
“So that is the main thrust of the argument. That’s one of the pieces of evidence that there is ongoing harm happening to us [because] they never stopped. To this day we are experiencing harm because of what New York City did to us. That was the real rationale that our attorneys were trying to get across.”
Unvaccinated teachers denied jobs due to the ‘problem code’
According to Combier’s affidavit, the DOE assigns “problem codes” to the personnel files of employees that “should not be hired due to unexplained misconduct of some kind.”
The affidavit stated:
“When the DOE puts a problem code in the employee’s personnel file, it also places a flag on the employee’s fingerprints, which is then sent to the national databases at both the Federal Bureau of Investigation and the State Division of Criminal Justice Services.
“I have represented more than 15 DOE employees before the DOE’s Office of Personnel Investigation in proceedings in which they requested the removal of their problem codes. The flag has several names such as ‘problem code,’ ‘pr’ code, ‘pc’ code, ‘ineligible,’ and ‘no hire/inquiry’ code; however, all refer to a salary block, whatever title it is given.”
Combier stated she had seen such “problem codes” in the personnel files of former DOE employees who did not receive the COVID-19 vaccine.
“The DOE places a problem code on the employee’s personnel file immediately upon getting information that the employee did not submit proof of vaccination.
“As soon as the employee gets the vaccination and submits proof, the code is removed from his or her file.”
Combier also provided an email from a DOE official confirming that a “problem code” was added to the personnel files of “DOE employees who were placed on leave without pay for failing to be vaccinated in violation of the DOE’s mandate.”
The “flag” then adversely impacted the employment prospects of teachers when they sought jobs outside of New York City. Combier wrote:
“I am aware that non-DOE schools located in counties outside New York City receive funds from the NYC DOE for certain teaching positions. These may include, for example, special education or STEM [science, technology, mathematics] teachers.
“The DOE pays the salaries for these positions using the same system it uses to pay traditional DOE employees, which is called Galaxy. Galaxy indicates whether the employee has a problem code in his or her file and blocks payment to the employee with this flag/code if viewed in the personnel file.”
As a result:
“At least 15 of my clients with problem codes were not hired by prospective schools outside the DOE because such schools saw the problem codes in Galaxy, even though those schools were located outside New York City.
“Such schools were able to see the codes because the position applied for was financed by the DOE and so the school used the Galaxy system and could check the prospective employee’s file.”
Attorneys for the city did not deny the veracity of this information in court.
Kane wrote, “Attorney Susan Paulson who was defending NYC stated that educators fired for declining COVID vaccination were not removed for misconduct, but rather for not meeting a requirement for employment.”
“If there was no misconduct, why are unvaccinated educators’ fingerprints sent to the FBI?” asked Kane.
Kane: Refusing vaccination isn’t ‘extremist’
Kane told The Defender that Teachers For Choice will attempt to work with city officials to discover the facts surrounding the assignment of the codes and the sharing of this information with the FBI, including determining who authorized these actions.
He told The Defender:
“The first thing we’re doing is we’re working with the Common-Sense Caucus in City Hall to get them to investigate. We need an investigation. I have my speculation of what’s going on, but the truth is we don’t know what’s going on. Who gave the order for these problem codes to be given simply for the fact that we’re declining COVID vaccination? Why did they do that? And have our civil rights been hurt because of it? I think they have.
“So right now, I think we need an investigation, because there’s lots of speculation happening and we need to get to the bottom of what really happened.”
The Common-Sense Caucus is an officially recognized caucus within the New York City Council.
Kane said it is composed primarily of Republicans and has “been the only voice against mandates in New York City governance.”
“We’ve been working closely with them, and they’ve been really pushing Mayor Eric Adams to be reasonable and to hear our concerns,” Kane said.
He said legal action is a strong possibility, but they will give Adams and the city an opportunity to respond first. He said:
“Right now we need to see if there will be any investigation into this, and we need to give New York City and Mayor Adams a chance to reply correctly. There’s a chance he didn’t do this. There’s a chance this happened from the previous administration, from Mayor Bill de Blasio.
“Letters need to be written, requests need to be made, and that may or may not lead to litigation. We have to see, because if the city complies and, and tries to work to fix this problem, I think that would be great. But we don’t know yet. It’s too early in the process.”
Kane also wrote that by sending biometric data about unvaccinated teachers to the FBI, “NYC educators were being set up to be viewed as ‘right-wing extremists’ or even ‘terrorists.’”
“Educators who declined COVID vaccination — including myself — had every right to do so,” Kane wrote. “No one is a ‘terrorist’ or ‘extremist’ for holding the line on what does and does not go inside of their bodies — especially injected directly into their muscle tissue,” he added.
Teachers fired by the DOE because they declined the COVID-19 vaccine may face a difficult time being rehired by the city, despite the city’s claims that such workers can reapply for employment now that the vaccine mandate for city employees has been rescinded.
Kane said “reapplication definitely could be problematic” for these individuals. But he also noted, “The city is bleeding for employees. They’re desperately dying for people to take jobs. So yes, I think it will hurt many, but I think the city is hurting way more right now.”
As previously reported by The Defender, the U.S. House of Representatives has convened a Select Subcommittee on the Weaponization of the Federal Government, investigating claims that agencies such as the FBI collected information on and in some cases harassed ordinary Americans for their beliefs on topics such as COVID-19.
Kane wrote that such practices in New York City are not new. DNA specimens of city employees collected from COVID-19 tests were cataloged in proprietary libraries owned by Fulgent Genetics, the company contracted by de Blasio to administer the tests. [MORE]
According to Dr Robert Malone the US Government is Tracking People Who Refused to Get COVID Shots or People Who Are Partially Jabbed through CDC Surveillance Program
/
Story at a glance:
The U.S. government has secretly been tracking those who didn’t get the COVID jab, or are only partially jabbed, through a previously unknown surveillance program designed by the U.S. National Center for Health Statistics, a division of the Centers for Disease Control and Prevention.
The program was implemented on April 1, 2022, and adopted by most medical clinics and hospitals across the U.S. until January 2023.
Under this program, doctors at clinics and hospitals have been instructed to ask patients about their vaccination status, which is then added to their electronic medical records as a diagnostic code, known as the International Classification of Diseases, Tenth Revision (ICD-10) code, so that they can be tracked inside and outside of the medical system.
These new ICD-10 codes are part of the government’s plan to implement medical tyranny using vaccine passports and digital IDs.
They’re also tracking noncompliance with all other recommended vaccines using new ICD-10 codes, and have implemented codes to describe WHY you didn’t get a recommended vaccine. They’ve also added a billable ICD code for “vaccine safety counseling.”
From [HERE] As recently discovered and reported by Dr. Robert Malone, the U.S. government has secretly been tracking those who didn’t get the COVID jab, or are only partially jabbed, through a previously unknown surveillance program designed by the U.S. National Center for Health Statistics (NCHS), a division of the Centers for Disease Control and Prevention (CDC).
The program was implemented on April 1, 2022, but didn’t become universally adopted by most medical clinics and hospitals across the U.S. until January 2023.
Under this program, doctors at clinics and hospitals have been instructed to ask patients about their vaccination status, which is then added to their electronic medical records as a diagnostic code, known as the ICD-10 code, without their knowledge or consent so that they can be tracked — not just within the health care system but outside of it as well.
Secret tracking program revealed
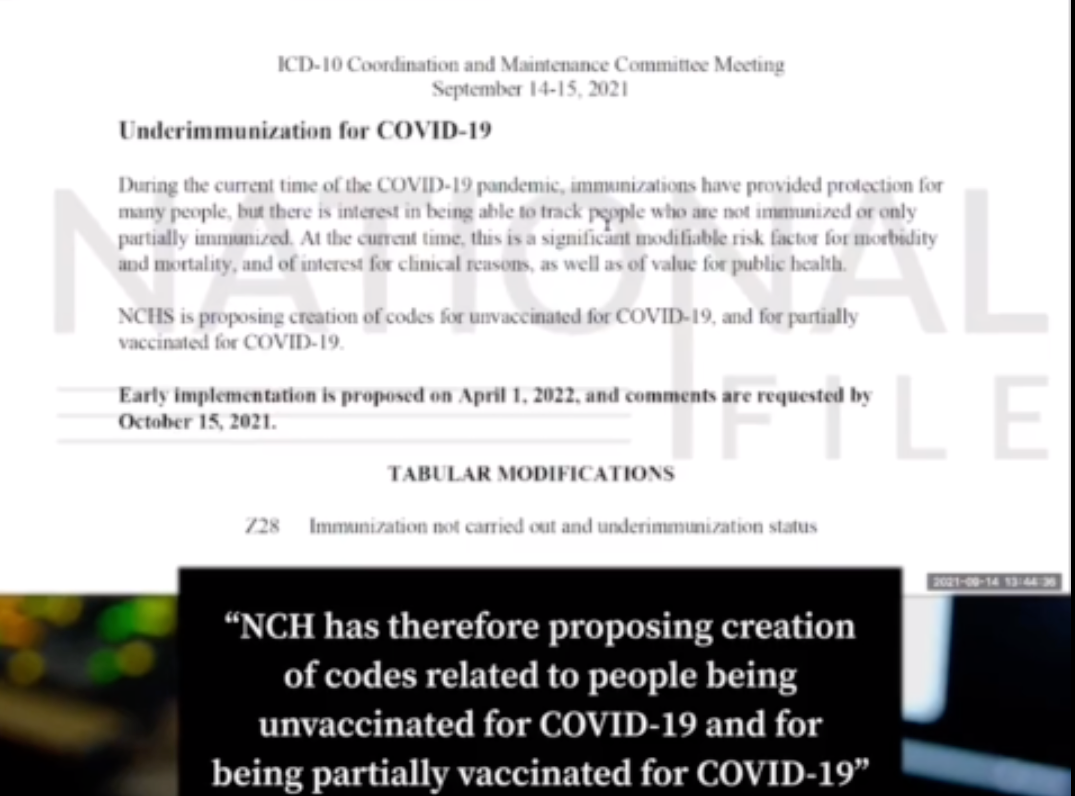
The new ICD codes were introduced during the Sept. 14-15, 2021, ICD-10 Coordination and Maintenance Committee meeting. The ICD committee includes representatives from the Centers for Medicare and Medicaid Services and the NCHS.
Below is a screenshot of page 194 of the agenda distributed during that meeting.
According to the NCHS, “there is interest in being able to track people who are not immunized or only partially immunized,” and they figured out a way to do just that, by adding new ICD-10 codes.
As you can see below, ICD-10 code Z28.310 identifies those who have not received a COVID jab and Z28.311 identifies those who are not up-to-date on their shots.
Tracking unjabbed is part of the biosecurity agenda
Why do they want to track the unvaccinated? For what purpose? The short answer: to facilitate the implementation of vaccine passports.
As noted by Malone:
“Code Number Z28.310 listed above is not a code for an illness or diagnosis, but rather for non-compliance of a medical procedure … Once a person’s vaccination status is coded and uploaded into large data base, it can be accessed by government and private health insurers alike.
“The administrative state officers at the CDC have not made immunization status a reportable disease (yet) but immunization status is listed as one of the reasons for mandatory reporting. They are just one step away from being able to collect this information without your permission. Ergo: vaccine passports made easy. In this country, not having your vaccine records ‘up-to-date’ might mean:
The government will not restrict your travel, airlines will.
The government will not restrict your travel, other nations will.
The government will not restrict your travel, auto rental companies will.
The government will not restrict your travel, public transport will.
The government will not restrict your travel, private companies will.”
World Health Organization signed off on tracking codes
The ICD codes were created by the World Health Organization (WHO) and doctors — with the exception of those in private practice who don’t accept insurance — are required to use these codes to describe a patient’s condition and the care they received during their visit. [MORE]
MIT Professor Retsef Levi Urges Governments to Stop All Experimental COVID Injections. ‘The Evidence is Mounting and Indisputable that mRNAShots are Causing Serious Harm Including Death’
/From [HERE] The number of health professionals urging for the suspension of COVID mRNA vaccine is increasing. The call for withdrawing the vaccine is getting stronger.
Recently, MIT Professor Retsef Levi took to Twitter to share the harm mRNA vaccines are causing in young people. "The evidence is mounting and indisputable that mRNA vaccines cause serious harm including death, especially among young people. We have to stop giving them immediately!," the MIT Expert in Analytics, Risk Management, Health Systems, Food & Agriculture Systems, Manufacturing & Supply Chain Management has tweeted.
Professor Levi's video, in which he has warned against the use of mRNA vaccine, has received more than 1 million views so far. “All COVID mRNA vaccination programs should stop immediately” “I’m filming this video to share my strong conviction that at this point in time, all COVID mRNA vaccination programs should stop immediately,” Professor Levi has said
“They should stop because they completely failed to fulfill any of their advertised promises regarding efficacy. And more importantly, they should stop because of the mounting and indisputable evidence that they cause unprecedented levels of harm, including the death of young people and children,” he continued.
“mRNA vaccines indeed cause sudden cardiac arrest”
“I believe that the cumulative evidence is conclusive and confirms our concern that the mRNA vaccines indeed cause sudden cardiac arrest as a sequel of vaccine-induced myocarditis. And this is potentially only one mechanism by which they cause harm,” he said.
“I personally became concerned with vaccine safety around the middle of 2021 when it became known that the mRNA vaccines cause myocarditis, and inflammation of the heart,” he says. “I was very concerned that it would not be detected by the existing vaccine safety surveillance systems. Motivated by that, we decided to analyze the Israel National EMS data to see if there are any signals of increased out of hospital adverse events,” he added and continued to substantiate his claims with the results of several studies.
“We detected an increase of 25% in the cause with cardiac arrest diagnosis”
“The analysis of the EMS calls and diagnosis data from 2018. throughout the first half of 2021 revealed some very concerning signals. We detected an increase of 25% in the cause with cardiac arrest diagnosis among ages 16 to 39. In the first half of 2021, exactly when the vaccination campaign in Israel was launched, a smaller increase was also detected in the older ages. Moreover, we also detected a statistically significant temporal correlation between the number of the Pfizer vaccine doses administered to this population and the number of EMS calls with cardiac arrest diagnosis,” says Professor Levi.
“Data from the UK, Scotland, and Australia replicate the data from Israel. Additional data from Israel indicates that in 2021, the EMS in Israel conducted more than 3,000 more resuscitations compared to 2019, which amounts for an increase of 27%. Two prospective studies from Thailand and Switzerland in which vaccines were tested before and after they received a vaccine, indicate that the rates of heart damage are likely to be significantly higher than the rates detected by clinical diagnosis. This is exactly the same finding that the US. military found in 2015 when it conducted a similar study on the smallpox vaccine.”
He continued, “Another study from the Harvard Medical School detected in the blood of children with vaccine-induced myocarditis, an entire spike, which is another indication of the underlying mechanism of harm, but in fact has even broader implications about the safety of the vaccine given the repeated evidence that we have that the mRNA and the lipids are actually penetrating the blood system.”
“And finally, autopsies of people that died closely after they received the vaccine indicate that in a large number of cases, there is strong evidence that the death was caused by vaccine-induced myocarditis. So presented with all of this evidence, I think there is no other ethical or scientific choice but to pull out of the market these medical products and stop all the mRNA vaccination programs. This is clearly the most failing medical product in the history of medical products, both in terms of efficacy and safety,” he said.
“This is huge”
Sharing Professor Levi’s video on his personal social media accounts, Dr Aseem Malhotra who has been vocal against the administration of mRNA vaccines has posted: "Eminent MIT Professor & expert on drug safety analytics Retsev Levi calls for immediate suspension of all covid mRNA vaccines
‘They should stop because they cause an unprecedented level of harm including the death of young people and children’
This is huge"
mRNA vaccines work by introducing a piece of a lab synthesized mRNA which corresponds to the viral protein. When the cells produce the viral protein using the mRNA an immune response is triggered. Not just COVID, mRNA vaccines have also been studied before for flu, Zika, rabies, and cytomegalovirus (CMV). Cancer research also uses mRNA to trigger the immune system to target specific cancer cells.
How do mRNA vaccines work?
A little portion of a protein typically located on the viral outer membrane is introduced as part of an mRNA vaccine's delivery mechanism. (People who receive an mRNA vaccination are not exposed to the virus and cannot contract the infection through the vaccine).
Here are the answers to few common questions related to mRNA vaccines:
What is mRNA vaccine?
mRNA vaccines use a piece of mRNA that corresponds to a viral protein.How to mRNA vaccines work?
These vaccines work by using laboratory synthesized mRNA to teach our cells how to make a protein to trigger immune response.What vaccines are mRNA?
Pfizer-BioNTech and the Moderna COVID-19 vaccines use mRNA .What are the other types of COVID vaccines available?
The other types of COVID vaccine available are vector vaccine and protein subunit vaccine.
Dr Nevradakis: Higher Infant Mortality Rates Linked to Higher Number of Vaccine Doses, New Study Confirms
/From [HERE] A new peer-reviewed study found a positive statistical correlation between infant mortality rates(IMRs) and the number of vaccine doses received by babies — confirming findings made by the same researchers a decade ago.
In “Reaffirming a Positive Correlation Between Number of Vaccine Doses and Infant Mortality Rates: A Response to Critics,” published Feb. 2 in Cureus, authors Gary S. Goldman, Ph.D., an independent computer scientist, and Neil Z. Miller, a medical researcher, examined this potential correlation.
Their findings indicate a “positive correlation between the number of vaccine doses and IMRs is detectable in the most highly developed nations.”
The authors replicated the results of a 2011 statistical analysis they conducted, and refuted the results of a recent paper that questioned those findings.
Miller spoke to The Defender about the study and its implications for infant and childhood vaccination schedules.
The more doses, the higher the infant mortality rate
In 2011, Miller and Goldman published a peer-reviewed study in Human and Experimental Toxicology, which first identified a positive statistical correlation between IMRs and number of vaccine doses.
The researchers wrote:
“The infant mortality rate (IMR) is one of the most important indicators of the socio-economic well-being and public health conditions of a country. The U.S. childhood immunization schedule specifies 26 vaccine doses for infants aged less than 1 year — the most in the world — yet 33 nations have lower IMRs.
“Using linear regression, the immunization schedules of these 34 nations were examined and a correlation coefficient of r = 0.70 (p < 0.0001) was found between IMRs and the number of vaccine doses routinely given to infants.”
In the above figures, “r” refers to the correlation coefficient, a number that ranges from -1 to 1. Any figure above zero is understood as a positive correlation, with figures between 0.6 and 0.79 considered a “strong” positive correlation, and 0.8 and above a “very strong” positive correlation.
The “p-value” indicates the extent to which the predictor’s value, in a linear regression analysis, is related to changes in the response variable.
A p-value of 0.05 or below is considered statistically significant, and indicative that the predictor and the response variable are related to each other and move in the same direction.
In the same 2011 study, which used 2009 data, the researchers found that developed nations administering the most vaccine doses to infants (21 to 26 doses) tended to have the worst IMRs.
“Linear regression analysis of unweighted mean IMRs showed a high statistically significant correlation between increasing number of vaccine doses and increasing infant mortality rates, with r = 0.992 (p = 0.0009),” the researchers wrote.
Miller told The Defender:
“In 2011, we published a study that found a counterintuitive, positive correlation, r = 0.70 (p < .0001), demonstrating that among the most highly developed nations (n = 30), those that require more vaccines for their infants tend to have higher infant mortality rates (IMRs).”
However, “critics of the paper recently claimed that this finding is due to ‘inappropriate data exclusion,’ i.e., the failure to analyze the ‘full dataset’ of all 185 nations.”
According to Miller:
“A team of researchers recently read our study and found it ‘troublesome’ that it’s in the top 5% of all research outputs. They wrote a rebuttal to our paper to ‘correct past misinformation’ and to reduce the impact of vaccine hesitancy.
“Their paper has not been published but it was posted on a preprint server.”
Miller said he and Goldman “wrote our current paper to examine the various claims made by these critics, to assess the validity of their scientific methods and to perform new investigations to assess the reliability of our original findings.”
The original paper studied the U.S. and 29 other countries with better IMRs “to explore a potential association between the number of vaccine doses … and their IMRs,” finding a strong positive correlation.
The 10 researchers — Elizabeth G. Bailey, Ph.D., a biology assistant professor at Brigham Young University, and several students associated with her Bioinformatics Capstone course who wrote the rebuttal to Goldman and Miller’s 2011 analysis — combined “185 developed and Third World nations that have varying rates of vaccination and socioeconomic disparities” in their analysis.
“One stated rationale behind Bailey’s reanalysis (and additional new investigations) is to reduce the impact of vaccine hesitancy, which ‘has intensified due to the rapid development and distribution of the COVID-19 vaccine,’” Goldman and Miller said. “They also appear to be targeting our study for a potential retraction.”
Miller explained the methodology Bailey’s team used:
“The critics select[ed] 185 nations and use linear regression to report a correlation between the number of vaccine doses and IMRs.
“They also perform[ed] multiple linear regression analyses of the Human Development Index(HDI) vs. IMR with additional predictors and investigate IMR vs. percentage vaccination rates for eight different vaccines.”
According to Miller, “Despite the presence of inherent confounding variables in their paper, a small, statistically significant positive correlation (r = 0.16, p < .03) is reported that corroborates the positive trend in our study (r = 0.70, p < .0001).”
In other words, there is still a positive correlation between the IMR and the number of vaccine doses, albeit weaker, among the 185 countries Miller’s critics studied.
However, this positive correlation is “attenuated in the background noise of nations with heterogeneous socioeconomic variables that contribute to high rates of infant mortality, such as malnutrition, poverty, and substandard health care” — meaning that there are confounding factors in poorer nations that significantly contribute to their higher IMRs.
Miller explained the difference in methodologies:
“We both used linear regression to analyze a potential correlation between the number of vaccine doses and IMRs. However, we analyzed the 30 most highly developed nations with high vaccination rates (consistently above 90%) and uniformity of socioeconomic factors.
“In contrast, our critics analyzed 185 nations with variable vaccination rates (ranging from less than 40% to greater than 90%) and heterogeneous socioeconomic factors.
“By mixing highly developed and Third World nations in their analysis, our critics inadvertently introduced numerous confounders. For example, malnutrition, poverty, and substandard healthcare all contribute to infant mortality, confounding the data and rendering the results unreliable.”
Miller and Goldman also conducted three other types of statistical analysis: odds ratio, sensitivity and replication analyses. These tests confirmed their findings, as they wrote in their new paper:
“Our odds ratio analysis conducted on the original dataset controlled for several variables. None of these variables lowered the correlation below 0.62, thus robustly confirming our findings.
“Our sensitivity analysis reported statistically significant positive correlations between the number of vaccine doses and IMR when we expanded our original analysis from the top 30 to the 46 nations with the best IMRs.
“Additionally, a replication of our original study using updated 2019 data corroborated the trend we found in our first paper (r = 0.45, p = .002).”
Put differently, the new study, which used 2019 data, found a somewhat weaker positive correlation of .045, but nevertheless confirmed a connection between the number of infant vaccine doses and IMRs.
Miller explained that, unlike the critics’ dataset of 185 countries, no adjustments for vaccination rates were necessary for his dataset, as “Vaccination rates in the countries that we analyzed generally ranged from 90-99%.”
He added that the odds ratio analysis considered 11 variables, including child poverty, and, “None of these variables lowered the correlation below 0.62.”
Similarly, said Miller, “In our sensitivity analysis, where we successively analyzed nations with worse IMRs than the United States, an additional 16 nations could have been included in the linear regression of IMRs versus the number of vaccine doses, and the findings would still have yielded a statistically significant positive correlation coefficient.”
Miller told The Defender the positive correlation he and Goldman identified grew stronger when the data were limited to highly developed countries:
“When we replicated our 2009 study using 2019 data, we once again found a statistically significant positive correlation between the number of vaccine doses and IMRs. Although the correlation was less robust (r = 0.45, p = .002) than our original finding, it corroborated the direction of the trend initially reported.
“When our 2019 linear regression analysis was limited to the top 20 nations, the correlation coefficient increased (r = 0.73, p < .0003), revealing a strong direct relationship between number of vaccine doses and IMRs.”
Miller noted that his conducted an additional analysis and based its conclusions on results it found for “high” and “very high developed nations” as categorized by HDI.
Their paper stated, “A re-analysis of only highly or very highly developed countries similarly shows that human development index (HDI) explains the variability in IMR, and more recommended vaccine doses does not predict more infant death.”
However, Goldman and Miller, in their new paper, challenged the use of HDI as a predictor of overall health in a country, noting that HDI looks only at “educational levels, income per capita, and life expectancy” and that multiple scholars have identified “severe misclassification in the categorization of low, medium, high, or very high human development countries.”
“As we discuss in our paper, up to 34% of HDI-classified nations are misclassified due to three sources of error, so it is unreliable,” Miller told The Defender. “Although our critics reported a strong correlation between HDI and IMR, this reveals no specific health measures that might be positively or negatively influencing IMR.”
Miller also noted, “An alternative index, the Human Life Indicator (HLI) was created to address HDI shortcomings. While Denmark was recently ranked fifth in the world by HDI, it fell to 27th place with HLI; the U.S. was recently ranked tenth by HDI while HLI ranked it 32nd.”
In summarizing the shortcomings of his critics’ study, Miller said:
“It was inappropriate for our critics to combine data from nations with highly variable vaccination rates and heterogeneous socioeconomic factors.
“In Third World nations, several factors contribute to a high infant mortality rate, thus when all 185 nations are analyzed (rather than limiting the analysis to the most highly developed homogenous nations), a positive correlation between number of vaccine doses and IMRs is attenuated or lost in the background noise of these other factors.”
Infant deaths spike in days following vaccination, data show
Miller previously studied the association between pediatric vaccines and sudden infant death, in a 2021 paper titled “Vaccines and sudden infant death: An analysis of the VAERS database 1990–2019 and review of the medical literature.”
Commenting on the findings of that research, Miller said:
“Of the 2,605 infant deaths reported to the Vaccine Adverse Event Reporting System (VAERS) from 1990 through 2019, 58% clustered within three days post-vaccination, and 78% occurred within seven days post-vaccination, confirming that infant deaths tend to occur in temporal proximity to vaccine administration.
“The excess of deaths during these early post-vaccination periods was statistically significant (p < 0.00001).”
Combined with the findings of his most recent paper, Miller argued that “Vaccines are not always safe and effective. Vaccine-related morbidity and mortality are more extensive than publicly acknowledged.”
He added:
“In all nations, a causal relationship between vaccines and sudden infant deaths is rarely acknowledged. Yet, physiological studies have shown that infant vaccines can produce fever and inhibit the activity of 5-HT [serotonin] neurons in the medulla, causing prolonged apneas and interfering with auto-resuscitation.”
Miller also highlighted the sequence in which vaccines are administered as a potential factor contributing to IMRs. He told The Defender:
“Global health officials do not test the sequence of recommended vaccines nor their non-specific effects to confirm they provide the intended effects on child survival. More studies on this topic are necessary to determine the full impact of vaccinations on all-cause mortality.
“In Third World nations, numerous studies indicate that DTP and inactivated polio (IPV) vaccines have an inverse safety profile, especially when administered out of sequence. Multiple vaccines administered concurrently have also been shown to increase mortality.”
Miller said that based on his latest study, “We do not know whether it is the vaccinated or unvaccinated infants who are dying at higher rates.” However, he noted most nations in his sample “had 90-99% national vaccination coverage rates.”
“In our paper, we provide plausible biological evidence that the observed correlation between IMRs and the number of vaccine doses routinely given to infants might be causal,” Miller said.
As a result, argued Miller, “more investigations regarding health outcomes of vaccinated versus unvaccinated populations … would be beneficial,” adding that “Health authorities in all nations have an obligation to determine whether their vaccination schedules are achieving desired goals.”
“Much more research needs to be done in this field, but more studies will only achieve limited positive change until more individuals and families begin to make the connection between vaccines and adverse events,” Miller said.
“Also, legislators and health authorities must permit people to accept or reject vaccines without intimidation or negative consequences.”
In 2021 More than 217,000 Americans Were Killed by Experimental COVID Injections
/
THE MEDIA IS TRYING TO KILL YOU
STORY AT-A-GLANCE
According to a December 2021 survey of 2,840 Americans, between 217,330 and 332,608 people died from the COVID jabs in 2021
Survey results also show that people who got the jab were more likely to know someone who experienced a health problem from COVID-19 infection, whereas those who knew someone who experienced a health problem after getting the jab were less likely to be jabbed
Of the respondents, 34% knew one or more people who had experienced a significant health problem due to the COVID-19 illness, and 22% knew one or more people who had been injured by the shot
51% of the survey respondents had been jabbed. Of those, 13% reported experiencing a “serious” health problem post-jab. Compare that to Pfizer’s six-month safety analysis, which claimed only 1.2% of trial participants experienced a serious adverse event
In December 2022, Rasmussen Reports polled 1,000 Americans. In this poll, 34% reported experiencing minor side effects from the jab and 7% reported major side effects
From [HERE] [PDF] While it's clear that the experimental COVID shots have killed a considerable number of people, the total death toll remains elusive, thanks to U.S. health agencies obfuscating, hiding and manipulating data.
That said, the most recent survey1,2 — published in the peer-reviewed journal BMC Infectious Diseases — puts the death toll from the COVID jabs somewhere between 217,330 and 332,608 in 2021 alone. As noted by Steve Kirsch:3
"[We've] killed at least 217,000 Americans and seriously injured 33 million … in just the first year, and the CDC and FDA want to give you more shots … Since deaths from the vaccine were higher in 2022, most experts would estimate the all-cause mortality death toll from the COVID vaccines to be in the range of 500K to 600K.
So the global cost of life from these vaccines is on the order of 10 to 12 million people … These [data] are consistent with the numbers I've been saying for a long time. It's not a coincidence."
Survey: Why People Did or Did Not Get the Jab
Now, the slant of this paper is kind of interesting. The primary aim of it was to "identify the factors associated by American citizens with the decision to be vaccinated against COVID-19."
The author was curious about why 31% of the U.S. population had declined the jab or not completed the primary series by November 2022, nearly two years into a massively advertised "vaccination" campaign.
Calculating the proportion of fatal events from the jab was secondary. As explained by the author, Mark Skidmore,4 Ph.D., an economics professor at Michigan State University:5
"A largely unexplored factor is the degree to which serious health problems arising from the COVID-19 illness or the COVID-19 vaccines among family and friends influences the decision to be vaccinated.
Serious illness due to COVID-19 would make vaccination more likely; the perceived benefits of avoiding COVID-19 through inoculation would be higher.
On the other hand, observing major health issues following COVID-19 inoculation within one's social network would heighten the perceived risks of vaccination. Previous studies have not evaluated the degree to which experiences with the disease and vaccine injury influence vaccine status.
The main aim of this online survey of COVID-19 health experiences is to investigate the degree to which the COVID-19 disease and COVID-19 vaccine adverse events among friends and family, whether perceived or real, influenced inoculation decisions. The second aim of this work is to estimate the total number of COVID-19 vaccine induced fatalities nationwide from the survey."
Here's an excerpt describing the methodology:6
"An online survey of COVID-19 health experiences was conducted. Information was collected regarding reasons for and against COVID-19 inoculations, experiences with COVID-19 illness and COVID-19 inoculations by survey respondents and their social circles. Logit regression analyses were carried out to identify factors influencing the likelihood of being vaccinated."
Survey Findings
A total of 2,840 people completed the survey between December 18 and 23, 2021. The mean age was 47, and the gender ratio was 51% women, 49% men. Just over half, 51%, had received one or more COVID jabs.
As Skidmore suspected, results showed that people who got the jab were more likely to know someone who experienced a health problem from COVID-19 infection, whereas those who knew someone who experienced a health problem after getting the jab were less likely to be jabbed.
Of the respondents, 34% knew one or more people who had experienced a significant health problem due to the COVID-19 illness, and 22% knew one or more people who had been injured by the shot. So, as noted by to the author:7
"Knowing someone who reported serious health issues either from COVID-19 or from COVID-19 vaccination are important factors for the decision to get vaccinated."
As for the types of side effects experienced by people within the respondents' social circles, they included (but were not limited to) the "usual suspects," such as:
Heart and cardiovascular problems
Severe COVID infection or other respiratory illness
Feeling generally unwell, weak, fatigued and out of breath for weeks
Blood clots and stroke
Death
Hundreds of Thousands Killed for No Reason
Based on these survey data, Skidmore estimates:
"… the total number of fatalities due to COVID-19 inoculation may be as high as 278,000 (95% CI 217,330-332,608) when fatalities that may have occurred regardless of inoculation are removed."
Were COVID-19 an infection with an extremely high mortality rate, perhaps high rates of death from a vaccine would be acceptable. But COVID-19 has an exceptionally low mortality rate, on par with or lower than influenza, hence the risk associated with the COVID jabs ought to be equally low.
The global cost of life from these vaccines is on the order of 10 to 12 million people. ~ Steve Kirsch
As it stands, the risks of the shots are very high, while Pfizer's own trial data, with more than 40,000 participants, show they offer no benefit in terms of your risk of hospitalization and/or death. The absolute risk reduction is so minute as to be inconsequential.8
High Rates of Side Effects
The death toll from the jabs isn't the only disturbing part of this paper, though. Skidmore's findings also suggest side effects from the jab may be more common than previously suspected.
As mentioned, 51% of the respondents had been jabbed. Of those, 15% reported experiencing a new health problem post-jab and 13% deemed it "serious." Compare that to Pfizer's six-month safety analysis,9 which claimed only 1.2% of trial participants reported a serious adverse event.
Now, as suggested by Kirsch,10 "we need to discount that by a factor of two because people report less severe adverse events as adverse events." Still, that means serious adverse events from the jab are five times higher than what Pfizer reported.
"This is why the FDA never does after-market surveys in the drugs it approves. Because reality hurts," Kirsch writes.11 "It is the FDA that should have discovered this before Mark Skidmore. The FDA is asleep at the wheel and they just believe everything the drug companies tell them, hook, line, and sinker. This is a major miss. Why aren't they doing surveys like this to see if the reality matches the study?"
More Side Effect Rate Comparisons
For additional comparison, here are the findings of several other investigations:
Rasmussen Reports12 — In December 2022, Rasmussen Reports polled 1,000 Americans. In this poll — taken one year after Skidmore's survey — 34% reported experiencing minor side effects from the jab and 7% reported major side effects.
CDC's V-Safe data13 — In October 2022, ICAN obtained the Center for Disease Control and Prevention's V-Safe data. This is a voluntary program to monitor adverse vaccine reactions. Of the 10.1 million COVID jab recipients who used the app, 7.7% had to seek medical care post-jab.
Kirsch-funded survey14 — A June 2022 U.S. survey by the market research company Pollfish found that 16.3% of COVID jabbed respondents experienced an injury, and 9.7% required medical care.
The graphic below, which visually compares Skidmore's findings to the findings of the Rasmussen, V-Safe and Pollfish surveys, was created by InfoGame on Substack.15 As noted by InfoGame:
"Skidmore's article serves as another sign that the rate of COVID-19 side effects is extremely high and that the COVID-19 vaccines are an unprecedently risky medical product."
- Sources and References
1, 5, 6, 7 BMC Infectious Diseases 2023; 23 article number 51
3, 10, 11, 19 Steve Kirsch Substack January 25, 2023
Damage control: Pfizer releases “urgent guidance” telling employees how to handle Project Veritas bombshell video
/From [HERE] Not long after Project Veritas released its latest bombshell exposé about Pfizer’s involvement in trying to manipulate covid to sell more “vaccines,” Google-owned YouTube pulled the video from its platform. Not long after that, the company issued an “urgent guidance” to its employees about how to handle the video whenever a user tries to upload or share it.
A screenshot of that urgent guidance – see below – informs YouTube employees that the Project Veritas video “violates the COVID-19 Vaccine Misinformation policy for making a categorical claim that COVID-19 vaccines are ineffective, and should therefore be removed unless it contains sufficient EDSA / CRC.”
YouTube is concerned about a specific timestamp in the video when it is stated by Project Veritas that “our undercover journalist asked Walker (referring to Jordon Trishton Walker) how Pfizer is handling the fact that their COVID vaccines are ineffective against virus variants.”
If that timestamp is present, then YouTube employees are to check the “[four] corners and metadata for EDSA that clearly contradicts, refutes or countervails the violative timestamp without any additional promotion (generalization, aggregation, repetition, affirmation).”
(Related: Check out our earlier coverage about Jordon Trishton Walker, a Boston Consulting Group [BCG] plant with a shady past who now works for Pfizer.)
If you’re going to share the Project Veritas bombshell video about Pfizer, be sure to follow the rules contained in the leaked YouTube “urgent guidance”
If a video upload of the Project Veritas video contains the offending timestamp and no sufficient CRC is present in the four corners, title, or description of the video, then YouTube employees are to issue a strike against the video and channel. [MORE]
Israelien Rulers Extend Irrational COVID Law Despite No Outbreak in Free Range Prison Disguised as Democracy
/From [HERE] Israel’s Knesset (parliament) Sunday renewed the Law on Special Authorities for Dealing with the Novel Coronavirus which grants the government unbridled authority to implement sweeping restrictions and criminalize non-compliance.
Despite there being no COVID-19 outbreak the law will remain in effect until February 15, 2024, "to continue to enable legal infrastructure for imposing restrictions and maintaining public health."
The law authorizes the government to require proof of vaccination, a negative coronavirus test or recovery certificate as a condition for entering places that are open to the public, businesses, workplaces, and more.
Restrictions may be placed on movement and gatherings both in public and private spaces, including one’s own residence. The government can close businesses and can force those that remain open to serve only the vaccinated.
Physical distancing and masking requirements may also be enforced.
Establishments allowing entry to a person who has not presented an up-to-date negative test result, Green Pass vaccine passport, or proof of recovery may be fined up to NIS 10,000 ($2,815).
The government may enforce hygiene, regulate types of activities and place restrictions related to a person’s private vehicle. Limitations on schools may be enforced as well.
“The law does not generally apply to the president of the state, official buildings of the Knesset, the state comptroller’s office, and courts and tribunals,” says the bill. “It similarly does not apply to the Israel Defense Force, the Israel police, the Prison Authority, and other institutions specified by the law.”
"Due to the uncertainty and the need for further monitoring of the corona disease, and especially against the background of the reports from China about the outbreak of the disease there, the minister accepted the recommendation of the professional officials at the Ministry of Health to extend the validity of the law,” Health Ministry officials told N12.
Acting Health Minister Yoav Ben-Zur reportedly signed the request to reinstate the law without officially consulting with the ministry.
The government notified the public of its proposal to renew the law and allowed public comment until January 13, 2023, but has ignored the overwhelming public opposition to the move.
Public Health Doctors Union Chairman Prof. Hagai Levin said: "We are not where we were three years ago, this is an unwillingness to give up the power and control that the authorities received during the COVID era.”
"This law is a draconian law that gives very broad powers to the ministry, cancels normal mechanisms of discussion in the Knesset and public discussion and may lead to misuse under the pretext of protecting public health in a disproportionate way,” he added.
Israel’s government drew heavily on these powers throughout the pandemic. Former Prime Minister Naftali Bennett, who accused the unvaccinated of "walking around with a machine gun firing Delta variants at people,” at one point proposed mandating bracelets which would publicly identify those who had not received the injections. He also proposed forcing the unvaccinated to pay for their own healthcare. Both proposals were supported by then-Health Minister Nitzan Horowitz though Bennett relented due to social pressure.
It was revealed last year that Israel's Health Ministry knew masks had 'no strong scientific basis' before imposing the mask mandate. Documents released under the freedom of information act revealed that Israel’s Health Ministry imposed the policy to send an “educational” message to increase COVID compliance.
Creating the Virus and “the Cure:” Coin-Operated RecogNegro Executive Tells Undercover Journalist Pfizer is Making COVID “Variants” to Infect People (gain of function research) to Sell More Injections
/
ACCORDING TO FUNKTIONARY:
RecogNegro – spotting a sell-out who has either crossed over or passed over into a reality that continuously crosses his or her kind out or passes them over to the “authorities” (racist economic and criminal injustice system). Everybody your color ain’t your kind or deeper still—all your skinfolks ain’t your kinfolks. (See: Afro-Sin-Trick, Sambo & Criss-Crossover)
coin-operated – the apt name for ravenous, puerile and greedy (“mine-controlled”) folk who only act if there is money, power or fame in the game (endeavor)—typically and consciously undertaken underhandedly at another’s expense. 2) anyone with a sell-out-slot that doubles as a mouth or who easily bends south—a south-bender repeat offender. 3) the subsumable drive for money, prestige, influence and power. 4) those that calculate and manipulate to get what they want— usually at the expense of others whom they claim to represent. 5) the description of (and name for) someone whose sole motivation is ‘paper-chasing.’ The living-larger supercilious sell-outs have to use the cracks of their arse as a discredit card swiper—since the stakes are higher and call for more drastic measures and high-volume transfers (the booty of sell-out treasures) can only be accessed in the form of plastic pleasures. They call them token Negroes because they are coinoperated. If you put money in them they will dispense (‘espew’—espouse and spew) the view, vision, wishes, ideas, thoughtforms, ideology, hopes and dreams of the customer [MORE]
biocide – the attempted annihilation of all life, which is the intent of Doggy and CrimethInc. (See: Doggy & CrimethInc.)

If SARS-CoV-2 is a Bioweapon, and the drug vaccine biologics (DVBs); viz. Pfizer, Moderna, & Janssen; make the SARS-CoV-2 Spike Protein, then doesn't it stand to reason that the DVBs are making part of the Bioweapons; & if it's a crime to make Bioweapons, then aren't the DVBs in violation of our treaties? [MORE]
Plandemic Profiteer Bill Gates Flip Flops on Experimental COVID Injections: Now Says so-called "Vaccines" Need to be Fixed b/c ‘They Aren’t Effective’
/
From [HERE] Bill Gates, long recognized as one of the world’s foremost proponents of vaccines, raised some eyebrows at a recent talk in Australia when he admitted there are “problems” with current COVID-19 vaccines.
Speaking at Australia’s Lowy Institute as part of a talk entitled “Preparing for Global Challenges: In Conversation with Bill Gates,” the Microsoft founder made the following admission:
“We also need to fix the three problems of [COVID-19] vaccines. The current vaccines are not infection-blocking. They’re not broad, so when new variants come up you lose protection, and they have very short duration, particularly in the people who matter, which are old people.”
Such statements came as a surprise to some in light of Gates’ longstanding support of — and investments in — vaccine manufacturers and organizations promoting global vaccination. However, they were the latest in a string of developments in recent weeks that have increasingly called the COVID-19 vaccines, in particular, into question.
‘This is a grift’: Gates’ investments in mRNA vaccines reveal ‘conflict of interest’
Several analysts and commentators were critical of Gates — but not due to disagreement with the statements he made in Australia. Instead, they argued that he had previously heavily invested in mRNA vaccines at the same time he encouraged a global COVID-19 vaccination campaign and supported mandatory vaccination.
Speaking Jan. 25 on The Hill TV’s “Rising,” co-hosts Briahna Joy Gray and Robby Soave addressed Gates’ statements. Soave initially agreed at face value with Gates’ criticism of current mRNA vaccines, saying:
“He really nails it on the issues that we’re having: the short duration of protection, not a significant discernable impact on the transmission of cases … not a massive benefit for a lot of otherwise healthy and younger people.”
However, Soave — who on Jan. 19 revealed “Facebook files” indicating the CDC significantly influenced content moderation and censorship on the platform pertaining to COVID-19 vaccines — then pointed out Gates’ prior investments that contributed to the development of mRNA vaccine technology.
Soave said, “Bill Gates was a major proponent of mRNA technology … he was an investor in BioNTech, which developed the mRNA vaccine for Pfizer.”
“We were just doing some digging,” continued Soave, “[and] we saw that he sold a lot of those shares at … how much profit was that?”
“10x,” replied Gray. “He invested $55 million in BioNTech back in 2019 and it’s now worth north of $550 million. He sold some stock … at the end of last year, I believe it was, with the share price over $300, which represented a huge gain for him over when he invested.”
Soave then unleashed critical comments directed at Gates:
“Let’s follow that trajectory: [Gates] invests heavily in BioNTech, ‘mRNA vaccines are great, this is the future,’ he talks about the vaccine timeline and how we can develop it faster, ‘we might have to cut some corners on safety’ … All in … sells it … makes a huge amount of money … but now it’s ‘yeah, it’s okay, it could be better, but what we really need is this breath spray.’”
Soave was referring to a statement Gates made during his recent talk in Australia, immediately prior to his remarks regarding the mRNA vaccines, where he said:
“We think we can also have, very early in an epidemic, a thing that you can inhale that will mean that you can’t be infected, a blocker, an inhaled blocker.”
Gray raised the issue of conflicts of interest between individuals such as Gates who hold significant positions with drug and vaccine manufacturers, and the federal government’s spending of large sums of taxpayer money to purchase these products. She said:
“This is a grift. These companies are extracting money, taxpayer money as it were, to pay for medical treatments that are not indicated by medical professionals and are less useful than what we already have.
“At the same time, the Biden administration is opening its doors, revolving doors, to people from these various industries like Jeff Zients, who is the new chief of staff for Joe Biden … who has spent his entire career at the kinds of companies, investing in the kinds of companies, that have been overcharging the government for Medicare and Medicaid payments and exact kinds of overpayments. It is an enormous grift and one that is incredibly common.”
Zients was formerly the Biden administration’s “COVID czar” and publicly pushed for universal vaccination.
Soave then said that Gates’ statements, and the broader issue of conflicts of interest between drug and vaccine proponents and the federal government, give credence to the assertions long made by “anti-vaxxers and the like.” He said:
“For there not to be more interrogation of his conflict of interest here by the mainstream is deeply disturbing, and for people who have been skeptical of this aspect of Pfizer and the drug development around COVID and who have been shot down in the media as kooks, anti-vaxxers and the like, I frankly think that this issue of pharmaceutical corruption and people pushing various interventions, having an investment in profit, should have been an issue that the left was leading on.
“We have to be more transparent about the fact that people who are having input in what the government policy is going to be, what’s going to be required people, the Biden administration tried to require people to get this, shouldn’t it be known at least when there are hundreds of millions of dollars of financial interests at stake for the people advising this? And their tune changes as it follows the money!”
Investigative journalist Jordan Schachtel also had scathing remarks following Gates’ statements in Australia, writing on his blog:
“Microsoft founder Bill Gates, who served as one of the architects of Covid hysteria and had more of an impact than any other individual on the disastrous global pandemic policies, has finally acknowledged that the mRNA shots he’s been promoting for two years are nothing more than expired pharma junk.
“Translation: Gates admits that the shots are impossible to align with rapidly developing variants, they expire in lighting speed, and they don’t stop transmission. And they don’t work for the only at-risk portion of the population.”
Schachtel called this “an incredible reversal from the man who once advertised the shots as the cure to the coronavirus,” drawing upon Gates’ previous statement: “everyone who takes the vaccine is not just protecting themselves but reducing their transmission to other people and allowing society to get back to normal.”
In 2021, Gates described the mRNA vaccines as “magic,” saying they would be a “game changer” in the next five years.
Gates warns about ‘next pandemic,’ praises lockdowns, calls for more pandemic simulations
As reported by the Daily Mail Jan. 23, Gates’ talk in Australia was notable for some additional statements he made.
Gates “called for greater global cooperation using the COVID-19 pandemic as an example of how countries could improve on their response if they worked together,” arguing that “political leaders needed to set aside their differences and work together to prepare for the next virus.”
He also praised Australia’s strict lockdown policies, saying:
“Some of the things that stand out are that Australia and about seven other countries did population scale diagnostics early on and had quarantine policies.
“That meant you kept the level of infection low in that first year when there were no vaccines.”
Gates also called for more “pandemic simulations” to assist world leaders in dealing with “future pandemics.” He said:
“The one thing that still hangs in the balance is will we have the global capacity and at the regional and country levels that would mean that when an (infectious disease) threat comes up we act in such a way that it doesn’t go global.
“We need to be doing every five years a comprehensive exercise at both country and regional levels of pandemic preparedness and you need a global group that’s scoring everybody.”
As part of such preparedness, Gates called upon countries to have “standby tools,” including vaccines, in place for the next pandemic:
“So there’s a class that’s got measles in it, a class of flu, a class of coronavirus, and a fourth class, all of which we need to have standby tools, both antivirals and vaccines that can deal with those. It’s very doable. So on the tools front, we can be far more prepared.”
Schachtel noted that Gates was a sponsor of Event 201, a simulation conducted Oct. 18, 2019, which “predicted” a global coronavirus pandemic. One of the sponsors of Event 201 was the Bill and Melinda Gates Foundation (BMGF).
The BMGF is a partner of Gavi, The Vaccine Alliance and holds a seat on its board. In turn, Gavi closely collaborates with the ID2020 Alliance, a strong proponent of “vaccine passports,” as previously reported by The Defender. Microsoft and the BMGF are founding members of ID2020.
According to the same report by The Defender, the BMGF in September 2022 pledged $1.27 billion in support of “global health and development projects.”
And as previously reported by The Defender, the BMGF previously committed, in June 2020, $750 million toward the development of the AstraZeneca vaccine at Oxford University, and conditional funding of $150 million to the Serum Institute of India — the world’s largest vaccine manufacturerby number of doses produced and sold.
The Serum Institute also received a $4 million grant from the BMGF in October 2020 to support research and development as part of the COVID-19 response, while in August 2020, the Serum Institute, in partnership with the BMGF and Gavi, agreed to produce up to 100 million doses of COVID-19 vaccines for low- and middle-income countries.
In a posting on his official blog in December 2020, Gates wrote that his foundation “took on some of the financial risk” for the vaccine, so that if the Oxford-AstraZeneca vaccine was not approved, the Serum Institute wouldn’t “have to take a full loss.” [MORE]

CDC Vaccine Safety Director: 'We are aware of these reports of people experiencing long-lasting health problems and Debilitating Illnesses following COVID Injections'
/From [HERE] CDC Immunization Safety Office Director Tom Shimabukuro admitted during an FDA advisory panel on Covid vaccines this week that his agency is aware of citizens suffering “debilitating illnesses” after taking the jabs.
“We take vaccine safety very seriously,” he said. “With respect to reports of people experiencing debilitating illnesses, we are aware of these reports of people experiencing long-lasting health problems following Covid vaccination.”
Shimabukuro continued, “In some cases the clinical presentation of people suffering these health problems is variable and no specific medical cause for the symptoms has been found. We understand illness is disruptive and stressful, especially under those circumstances, and we acknowledge these health problems have substantially impacted the quality of life for people and have also affected those around them.”
“We hope for improvement and recovery and we will continue to monitor the safety of these vaccines and work with partners to better understand these types of adverse events,” he added. [MORE]
FDA Probes Higher Risk of Stroke When Covid Booster, Flu Jab Taken on Same Day –as Recommended by the Blight House
/From [HERE] The FDA is looking into whether there’s an increased risk of stroke after taking a flu jab and Covid booster vaccine on the same day, advice that was promoted by the White House.
The federal agency revealed the investigation after an analysis found “seniors who received both the Pfizer omicron booster and a high-dose or adjuvanted flu vaccine on the same day may have a higher risk of stroke,” CNBC reported Thursday.
“Although the FDA has not identified a stroke risk, the agency is launching a study to examine potential safety concerns that may arise from administering the Covid omicron shots at the same time as the high-dose or adjuvant flu shots,” reported CNBC citing FDA biostatistics deputy director Richard Forshee.
The investigation comes as “Millions of Americans got both shots at the same time this winter following a major public health push by the White House,” according to the Daily Mail.
Heading into winter, Biden’s White House Covid response coordinator Ashish Jha urged Americans on at least two occasions to inject both jabs simultaneously.
“The good news is you can get both your flu shot and Covid shot at the same time. It’s actually a good idea. I really believe this is why God gave us two arms; one for the flu shot and the other one for the Covid shot,” Jha told Americans during a Covid-19 Response Team press conference in September. [MORE]
Cardiologist Dr Thomas Levy: Over 7M Americans may have some form of Heart Injury Due to COVID Injections
/From [HERE] Board-certified internist and cardiologist Dr. Thomas Levy told Steve Kirsch in an interview on Jan. 17 that over seven million Americans may be suffering from some degree of heart damage because of the Wuhan coronavirus (COVID-19) vaccines.
Levy came up with these startling figures based on the assumption that at least 2.8 percent of people who get the COVID-19 vaccines eventually developed some form of heart injury detectable with a troponin test. (Related: EVERYONE who gets mRNA jabbed for covid suffers some degree of heart injury, study finds.)
Official data released on August 21, 2022, showed a total of 263 million Americans, or 79 percent of the U.S. population, have received at least one dose of COVID-19 vaccine. Given those figures, the projected number of Americans with vaccine-induced heart damage would be around 7.4 million.
A prolific book author, Levy recently published an essay titled “Myocarditis: Once Rare, Now Common,” which formed the basis of his discussion with Kirsch on the excess deaths occurring in the United States that could be attributed to the mRNA injections.
Among the salient points covered by the essay was the relationship between COVID-19 and myocarditis, or inflammation of the heart muscle. According to Levy, “scientific literature indicates that myocarditis is occurring quite frequently in patients harboring the chronic presence of the spike protein.”
According to Levy, an elevated troponin level on blood testing is extremely sensitive in picking up any ongoing heart muscle cell damage. “Some elevation of this test will always be seen if any significant inflammation is present in those muscle cells.”
Levy mentioned a recent Swiss study yet to be published, which measured troponin levels on 777 hospital employees who got boosted after two injections. On the third day after the booster, troponin levels above the upper limits of normal were seen in 2.8 percent of those subjects. By the next day, however, half of the elevated troponin levels had returned to normal.
As expected, the study authors dismissed the probability that some myocardial damage was done by the vaccine. However, Levy thinks incidents like death on the playing field by physically fit European football players in the last two years indicate that something unusual is going on among vaccinated individuals.
These sudden deaths should pose serious concerns, but are largely ignored by the government and the mainstream media because they contradict the COVID narrative they are trying to espouse.
COVID-19 vaccine rollouts trigger spike in excess deaths everywhere
Recent studies in various countries like Australia, Japan, New Zealand, Israel and the Netherlands have shown similar patterns of increased excess deaths following rollouts of COVID-19 vaccines.
Levy also cited a study in mice showing that the mRNA vaccines, which produce spike proteins, can induce myopericarditis – a complication of acute pericarditis. “Regardless of the initial source of exposure to spike protein, it appears to be the reason for the pathology and symptoms seen in chronic COVID.”
Worse, Levy believes mRNA vaccine shedding is possible.
“Once transmitted, the mRNA directly leads to spike protein production. Such mRNA shedding means that the spike protein is indirectly, if not directly as well, transmissible from one individual to another via inhalation or various forms of skin contact,” he noted.
Another topic discussed during the Kirsh interview was the heart damage in vaccinated pilots caused by the vaccines. This surfaced after the Federal Aviation Administration (FAA) made some adjustments in its guidelines, possibly because of the huge number of pilots failing routine health screenings.
In October 2022, the FAA widened the ECG parameters beyond the normal range – from a PR max of 0.2 to unlimited. Levy said this is a “tacit admission from the U.S. government that the COVID vaccine has damaged the hearts of American pilots.”
“The cardiac harm, of course, is not limited to pilots. My best guess right now is that over 50 million Americans sustained some amount of heart damage from the shot,” Kirsch remarked. [MORE]