"No Deaths Can be Said to Have Been Averted Due to Vaccination." According to a Study of Data from All States in All Age Groups, COVID Injections Had No Impact on Reducing Deaths from COVID
/
COVID-Period Mass Vaccination Campaign and Public Health Disaster in the USA. From age/state-resolved all-cause mortality by time, age-resolved vaccine delivery by time, and socio-geo-economic data
By Denis G. Rancourt PhD, Marine Baudin, PhD, Jérémie Mercier, PhD
ABSTRACT
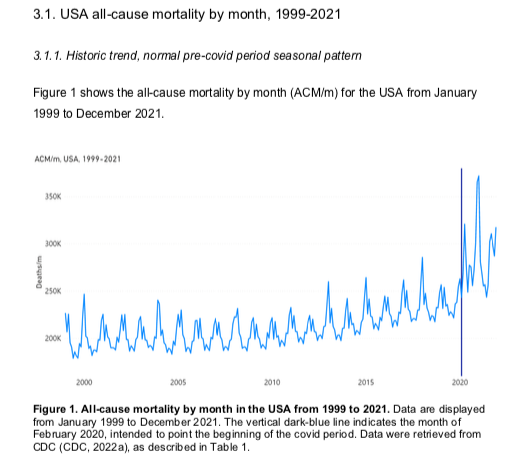
From [HERE] and [HERE] All-cause mortality by time is the most reliable data for detecting and epidemiologically characterizing events causing death, and for gauging the population-level impact of any surge or collapse in deaths from any cause. Such data is not susceptible to reporting bias or to any bias in attributing causes of death. We compare USA all-cause mortality by time (month, week), by age group and by state to number of vaccinated individuals by time (week), by injection sequence, by age group and by state, using consolidated data up to week-5 of 2022 (week ending on February 5, 2022), in order to detect temporal associations, which would imply beneficial or deleterious effects from the vaccination campaign. We also quantify total excess all-cause mortality (relative to historic trends) for the entire covid period (WHO 11 March 2020 announcement of a pandemic through week-5 of 2022, corresponding to a total of 100 weeks), for the covid period prior to the bulk of vaccine delivery (first 50 weeks of the defined 100-week covid period), and for the covid period when the bulk of vaccine delivery is accomplished (last 50 weeks of the defined 100-week covid period); by age group and by state.
We find that the COVID-19 vaccination campaign did not reduce all-cause mortality during the covid period. No deaths, within the resolution of all-cause mortality, can be said to have been averted due to vaccination in the USA. The mass vaccination campaign was not justified in terms of reducing excess all-cause mortality. The large excess mortality of the covid period, far above the historic trend, was maintained throughout the entire covid period irrespective of the unprecedented vaccination campaign, and is very strongly correlated (r = +0.86) to poverty, by state; in fact, proportional to poverty. It is also correlated to several other socio-economic and health factors, by state, but not correlated to population fractions (65+, 75+, 85+ years) of elderly state residents.
The excess all-cause mortality by age group (also expressed as percentage of pre- covid-period all-cause mortality for the age group) for the whole USA for the entire covid period through week-5 of 2022 is:
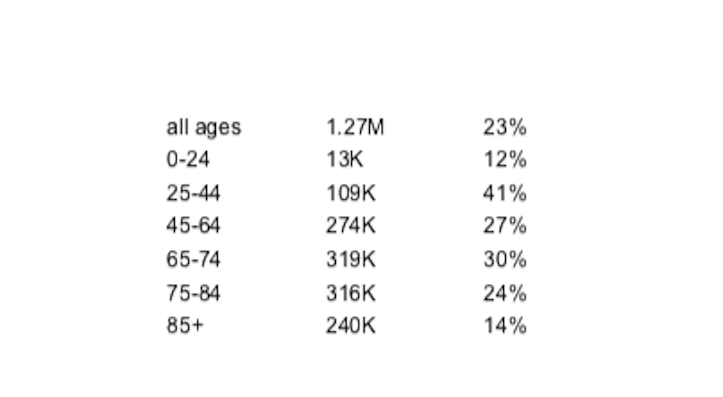
The corresponding fatality risk ratios are relatively uniform with age (non-exponential and non-near-exponential with age; and even skewed towards young adults), which holds essentially for all states, and for all examined periods within the covid period. This fundamental result implies that a dominant cause of excess mortality could not have been assigned COVID-19, which consistently has been measured to have a strong near-exponential infection fatality ratio with age. The implication is further corroborated by the absence of correlation between all-age-group-integrated excess mortality and age, by state. COVID-19 was not a dominant cause of excess mortality during the covid period in the USA
All of our observations can be coherently understood if we interpret that the covid-period socio-economic, regulatory and institutional conditions induced chronic stress and social isolation among members of large vulnerable groups (individuals afflicted and co- afflicted by poverty, obesity, diabetes, high susceptibility to bacterial respiratory infection [inferred from pre-covid-period antibiotic prescription rates], old age, societal exclusion, unemployment, drug and substance abuse, and mental disability or serious mental illness), which in turn caused many of these individuals to be more and fatally immunocompromised, allowing them to succumb to bacterial pneumonia, at a time when a documented national pneumonia epidemic raged and antibiotic prescriptions were systemically reduced; in addition to possible comorbidity from COVID-19 vaccine challenge against individuals thus made immunocompromised, under broad and hastily implemented “vaccine equity” programs. [MORE]